Table of Contents
- Key Takeaways
- Introduction
- Farmworkers’ Changing Health and Demographics
- Changing Policies for Providing Health Insurance
- Barriers to Health Care for Farmworkers
- Health Services Used by Farmworkers
- Insurance Coverage Patterns after Policy Changes
- Fewer Cost or Insurance Concerns for Documented Immigrants
- Conclusion and Recommendations
- Notes and References
- Authors and Acknowledgments
- PPIC Board of Directors
- Copyright
Key Takeaways
Recent federal and state policies may have improved access to health insurance for farmworkers, who are important contributors to California’s economy and an essential link in the food supply chain. The Affordable Care Act (ACA) included an expansion of Medi-Cal to most low-income adults, and a mandate requiring companies with at least 50 workers to offer employer health insurance. California also expanded Medi-Cal to young undocumented immigrants, and will soon extend it to older individuals. This report investigates whether these policies coincided with better insurance coverage or reduced barriers to health care for immigrant farmworkers.
- Farmworkers are aging and more likely to settle in the US with family; thus, their health care needs—and those of their families and children—will likely grow. →
- Cost or lack of insurance are the most salient barriers to health care for farmworkers; few farmworkers note barriers related to immigration status, although being undocumented is a strong predictor of lacking health insurance. →
- Many documented farmworkers have enrolled in Medi-Cal following the ACA expansion, which has increased coverage rates and lowered cost and insurance barriers to health care. Undocumented farmworkers have not fared as well in these areas. →
- Employer health insurance coverage for farmworkers did not change detectably with the rollout of the ACA employer mandate, regardless of a farmworker’s documentation status or whether the worker was a direct hire versus a contractor. →
These findings take on special importance during the coronavirus pandemic. Farmworkers have continued to work during the public health emergency. Yet with California’s high cost of housing, many farmworkers live in crowded conditions, making it difficult to remain socially distant from other household members. Although emergency Medi-Cal covers COVID-19 treatment regardless of immigration status, long COVID and resulting disability may threaten farmworkers’ health and livelihoods.
Introduction
About 162,500 farmworkers worked in California in 2019, according to estimates from the American Community Survey, but their relatively small numbers contrast with their significant contributions. These workers are a key link in the food supply chain in California and nationwide. Farmworkers play an important role in the state’s agricultural economy, a sector that produced over $50 billion in revenue in 2019 (California Department of Food and Agriculture 2020a), with California’s crop sales recently accounting for 17 percent of the US total (US Department of Agriculture 2017).
California is the leading state in terms of agricultural revenues, and is the sole producer of a number of products, including almonds, walnuts, plums, and figs (California Department of Food and Agriculture 2020a). Over three-fourths of California’s crop sales are fruits, nuts, and vegetables (California Department of Food and Agriculture 2020a), many of which depend on farm workers for production and harvesting.
While many individuals switched to working at home during the COVID-19 pandemic, most farmworkers continued their essential, in-person work. A recent California study detailed farmworkers’ fears of catching the coronavirus at work, compounded by lack of access to health care and social services, and their need to work in order to survive economically (California Institute for Rural Studies 2021). In the years leading up to the pandemic, a number of federal and state policy changes may have helped improve access to health care for farmworkers.
The Affordable Care Act (ACA), a major reform of the US health system, allowed California to expand Medi-Cal public health insurance to low-income residents beginning in 2014, and required large employers to offer health insurance to their workers beginning in 2015. Additionally, California implemented Medi-Cal expansions primarily funded with state dollars to cover low-income undocumented young adults in 2020; an expansion to undocumented older adults will begin later this year. This series of policy changes may have improved access to health insurance and health services for farmworkers, who are overwhelmingly immigrants, and many of whom are low-income. A further expansion proposed in Governor Newsom’s January 2022 budget would cover low-income adults ages 26–49, regardless of immigration status.
I analyze federal survey data to determine whether the timing of new policies were associated with changes to insurance and barriers to care for farmworkers. I also conducted expert interviews to provide additional key context (see textbox on data sources). This report focuses on a subset of California farmworkers in crop agriculture whose employers allow government surveyors to interview their workers, and who do not hold guest worker (H-2A) visas. From here on, I refer to immigrant farmworkers without guest worker visas as just “farmworkers” for brevity.
In this report, I describe farmworkers’ characteristics, changes (if any) to their health insurance options, and their barriers to health care. I also discuss some differences among farmworkers by crop type, employer type, and geography. Throughout, I focus on immigrant farmworkers, who make up more than 90 percent of California farmworkers, and pay particular attention to undocumented workers—those without valid visas or permanent residency (“green cards”)—who make up over half of immigrant farmworkers (Figure 1, and Technical Appendix Table A1 and Table A2). Undocumented immigrants likely have additional barriers to health insurance coverage and health services; past research in California finds these patterns (Cha and McConville 2021). This group of workers also may have other characteristics that affect their health needs.
The overwhelming majority of California’s farmworkers are immigrants, and over half are undocumented
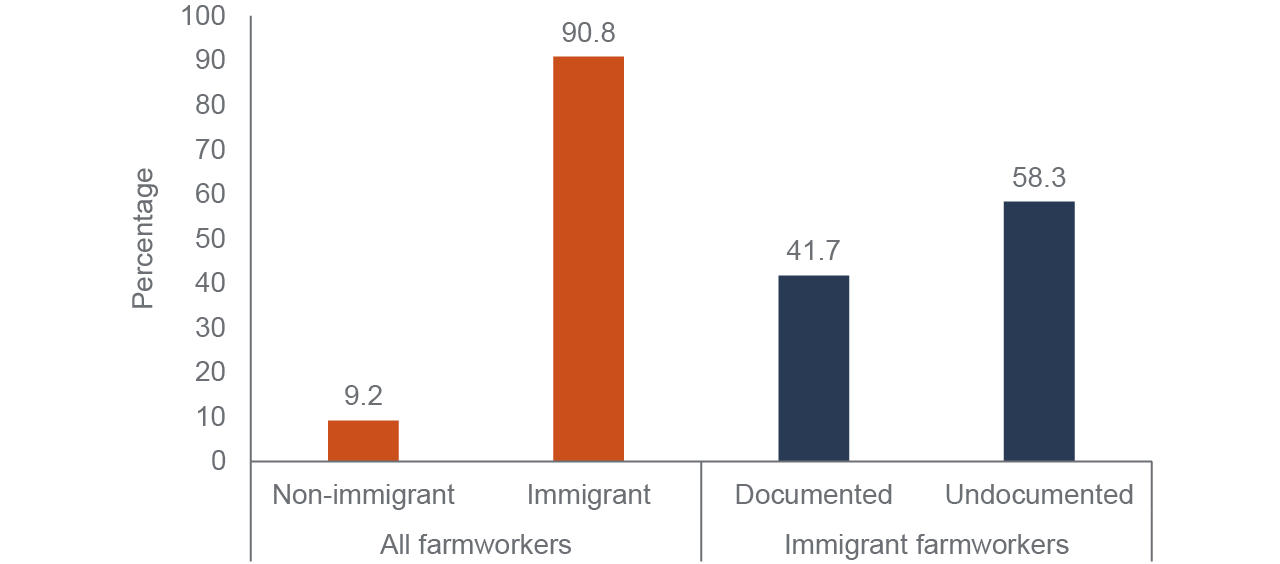
SOURCE: National Agricultural Workers Survey, fiscal years 2010–2018.
NOTE: Weighted tabulations presented. All farmworkers includes California survey participants. Immigrants are those born outside of the United States and Puerto Rico. Documentation status is self-reported in the survey.
Farmworkers’ Changing Health and Demographics
The profile of farmworkers has been changing over time, and their health needs are likely to have grown as a result. Currently, about 70 percent of California farmworkers are male, and about 97 percent are Latino (Technical Appendix Table A1 and Table A2). Ninety-two percent are Spanish speakers and 44 percent report they do not speak English. Farmworkers tend to have low levels of formal education: about 74 percent did not complete high school, and 93 percent have at most a high school diploma or equivalent. In light of these characteristics, language, low education, and low income are likely common barriers to health care for farmworkers. Language may be especially a barrier for Indigenous farmworkers (see Technical Appendix C for more). Farmworkers also participate in highly physical work that can lead to injuries (Cha 2021; Zavodny 2015), making the need for health care access pressing.
A trend taking shape over decades is the increasingly settled nature of farm work, with workers living in the United States year-round. In the past, patterns of settling were quite different by immigration status (Figure 2). Documented immigrants tended to be settled, while undocumented immigrants were more likely to travel to the US to work and regularly return home for periods of respite.
Around 2010, both groups converged to a relatively low level of international shuttling, as the practice is called. Undocumented farmworkers moving less could be a response to increased border control, which is correlated with lower labor migration (Fan et al. 2015) and longer stays by undocumented immigrants (Reyes, Johnson, and Van Swearingen 2002). Regardless of the root causes, farmworkers are now mainly a settled group of long-time residents and workers.
Since 2010, California’s undocumented and documented farmworkers have had similar international movement
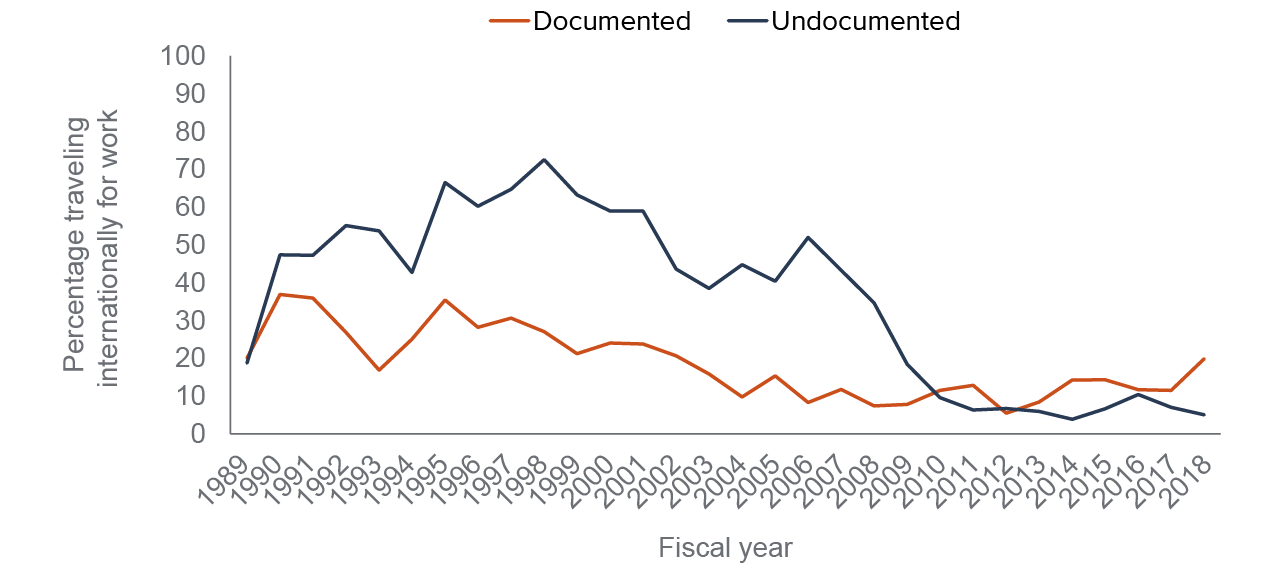
SOURCE: National Agricultural Workers Survey, fiscal years 1989–2018
NOTE: Weighted averages presented. Farmworkers include California survey participants, and immigrants are those born outside of the United States and Puerto Rico. International shuttling refers to working in the US but spending at least 28 days abroad a year (excluding daily border crossing). Undocumented status is self-reported.
A consequence of settling is that workers are now living with their families in the US instead of keeping their families in their countries of origin (Hamilton and Hale 2016); for example, farmworkers are increasingly living with their spouses (Figure 3).
The question of access to care then becomes one about families and children, not just about lone workers whose permanent homes are elsewhere. Although farmworkers are mostly male (Technical Appendix Table A1 and Table A2), having families in the US means that women’s health concerns, prenatal care, and pediatric services become more salient needs. Documentation status can differ within families as well; over a quarter of farmworkers report being in a mixed-status family. That is, different family members may be documented, undocumented, or US citizens.
While a settled lifestyle may work well for connecting farmworkers to a clinic as a regular source of care, one expert I spoke with mentioned that even small changes in work site location could raise challenges to consistent care since many farmworkers carpool and do not have access to private transportation. Contract workers could be sent to different counties regularly, creating an unsettled day-to-day work life. Another expert noted that some workers prefer to get care in Mexico rather than in the US, so being settled does not necessarily preclude getting health care abroad.
Increasingly, immigrant farmworkers in California live with their spouses
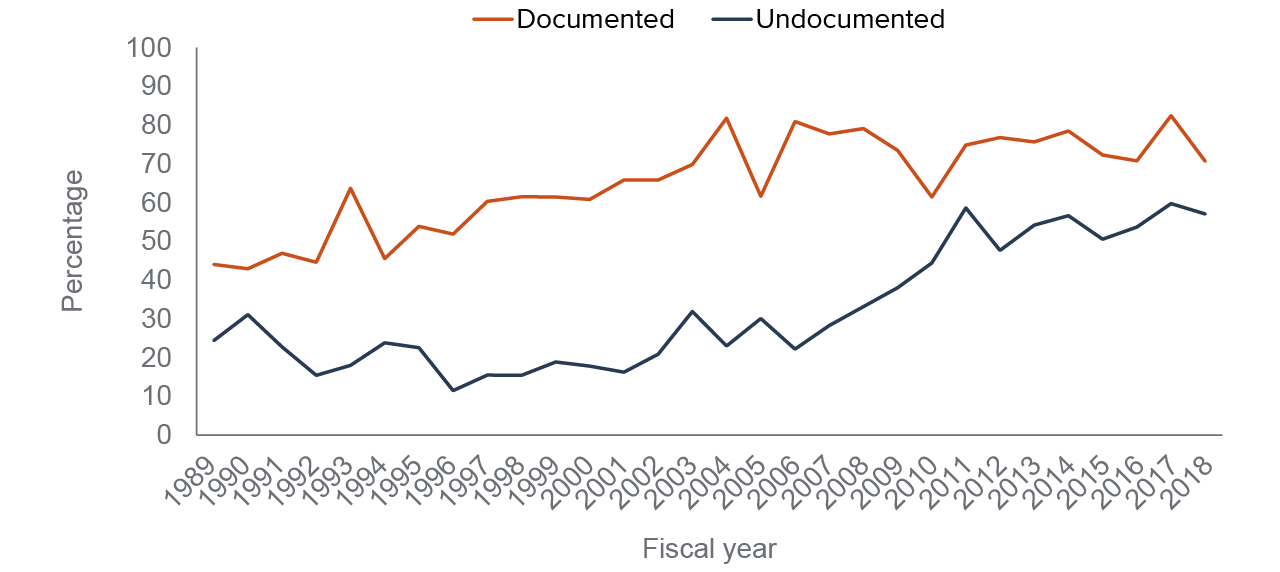
SOURCE: National Agricultural Workers Survey, fiscal years 1989–2018
NOTE: Share of farmworkers residing with spouses shown. Weighted averages presented. Farmworkers include California survey participants, and immigrants are those born outside of the United States and Puerto Rico. Undocumented status is self-reported.
As farmworkers have become a settled workforce in the US, they have been aging; the average farmworker is now over 40 years old. Undocumented workers have tended to be younger than their documented counterparts, but they, too, are getting older (Figure 4). Older individuals will have greater health care needs, elevating the importance of addressing health care barriers among farmworkers and their family members.
Age also comes with a need for various preventive screenings that are not typically recommended for younger individuals. Those with undiagnosed conditions or who lacked access to care in the past can face negative health consequences in older years. For example, Sonoma County farmworkers mostly working in wine grapes had much higher rates of diagnosed diabetes compared to the county average (18% vs. 5%), and self-described fair or poor health (44% vs. 13%) (Moore et al. 2016).
In California, undocumented immigrants over age 50 are much less likely to have health insurance compared to documented immigrants (51% vs. 91%) (Cha and McConville 2021). The lack of insurance may be problematic for older farmworkers, especially those who will not be eligible for Medicare when they turn 65. Without insurance, these older adults may not have an affordable way to pay for their increasing health needs. One expert I interviewed emphasized that long-term care is a growing concern among aging farmworkers.
The average age of immigrant farmworkers has increased
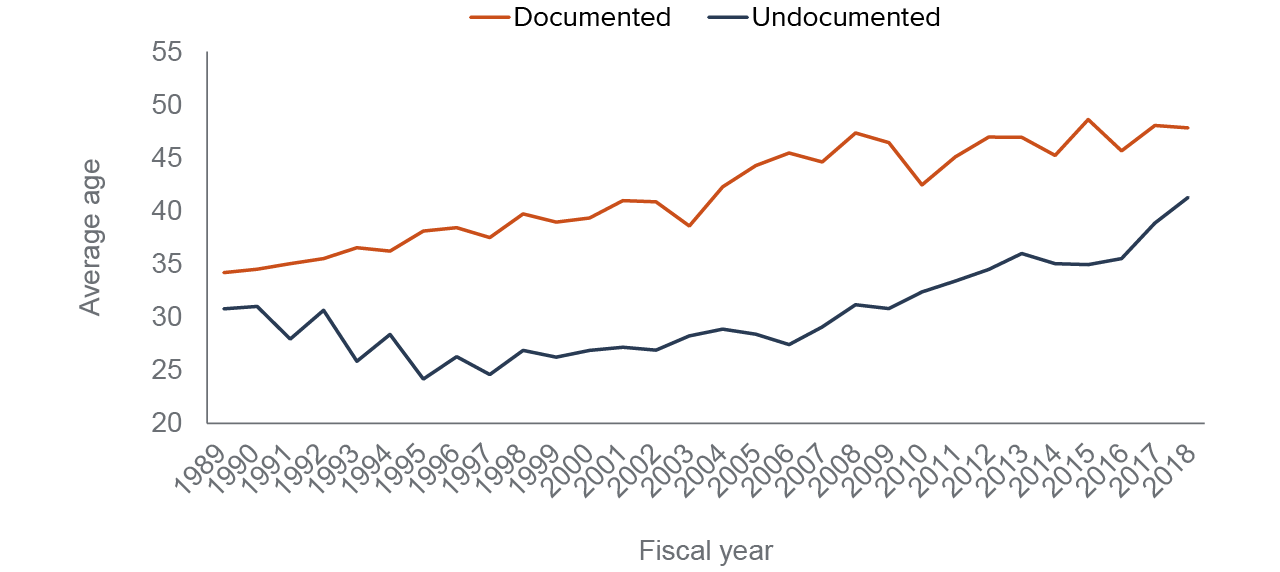
SOURCE: National Agricultural Workers Survey, fiscal years 1989–2018
NOTE: Weighted averages presented. Farmworkers include California survey participants, and immigrants are those born outside of the United States and Puerto Rico. Undocumented status is self-reported.
Changing Policies for Providing Health Insurance
The federal Patient Protection and Affordable Care Act of 2010, known as the ACA, expanded health insurance coverage, though most of its provisions do not apply to undocumented immigrants. In 2014, California expanded Medi-Cal, the state’s Medicaid program (McConville and Cha 2019), to a broad population of low-income adults under the ACA.
Documented farmworkers who earn incomes less than 138 percent of federal poverty are now eligible to enroll in the program, but undocumented farmworkers have generally remained ineligible. The expansion does allow undocumented immigrants to access a version of Medi-Cal that covers medical emergencies and pregnancy-related services, and Medi-Cal covers specific conditions regardless of immigration status, but most undocumented immigrants are ineligible for comprehensive coverage.
The ACA also included an employer mandate, which required that employers with at least 50 full-time employees (or their equivalent) offer employer-supplied insurance to their workers (see Technical Appendix Figure A1 for how ACA provision years align with the years in this report’s analysis). Although most provisions of the ACA, namely the Medicaid expansion and marketplaces for purchasing non-group private coverage, exclude undocumented immigrants, employer insurance is not limited in the same way. As a result, the employer mandate could improve coverage for farmworkers regardless of their immigration status.
Another important ACA provision was to establish health care marketplaces where individuals can purchase private health insurance, and low-income individuals can receive government subsidies. Covered California is the state’s marketplace, and it now enrolls about 1.8 million residents. However, this is a small proportion of the state’s population, which is close to 40 million, and data limitations make it infeasible to detect the effects of the marketplace in this study.
Preliminary analyses before the employer mandate was implemented suggested that farmworkers would be left out of this expansion or would be difficult to track (Guild, Richards, and Ruiz 2016; Kissam 2014). Below, I address the effects on farmworkers now that the employer mandate has been in place for several years.
State Medi-Cal Expansions Focused on Undocumented Immigrants
In California, almost 1.3 million undocumented adults under age 65 were uninsured in 2022, making up an estimated 40 percent of the state’s uninsured individuals in this age group (Dietz et al. 2021). California policymakers have been responding by implementing expansions of Medi-Cal using mostly state funds. In May 2016, SB 75 extended Medi-Cal eligibility to low-income children under age 19, regardless of immigration status (California Legislative Information 2020). This was followed by SB 104, which used a similar approach to expand Medi-Cal to young adults under age 26, regardless of immigration status.
These state policies covered the youngest, and therefore, the least expensive age groups. In a deal between Governor Newsom and members of the legislature, California included a further expansion of Medi-Cal to undocumented older adults in the 2021 budget trailer bill. This latest policy change will take effect in May 2022, when California will expand Medi-Cal to all individuals ages 50 and over who meet income eligibility requirements regardless of immigration status. This age group has been growing as a proportion of the undocumented farmworker population in recent years (Figure 5).
The older adults are a relatively small, but expensive, group to cover. The expansion budget for these individuals includes funds for In-Home Support Services (IHSS), a Medi-Cal program that pays caregivers to help enrollees live independently (Beck 2015). The IHSS provision helps address the need for long-term care options for older undocumented farmworkers.
Nearly one-fifth of undocumented farmworkers will be affected when Medi-Cal expands to those age 50+ in 2022
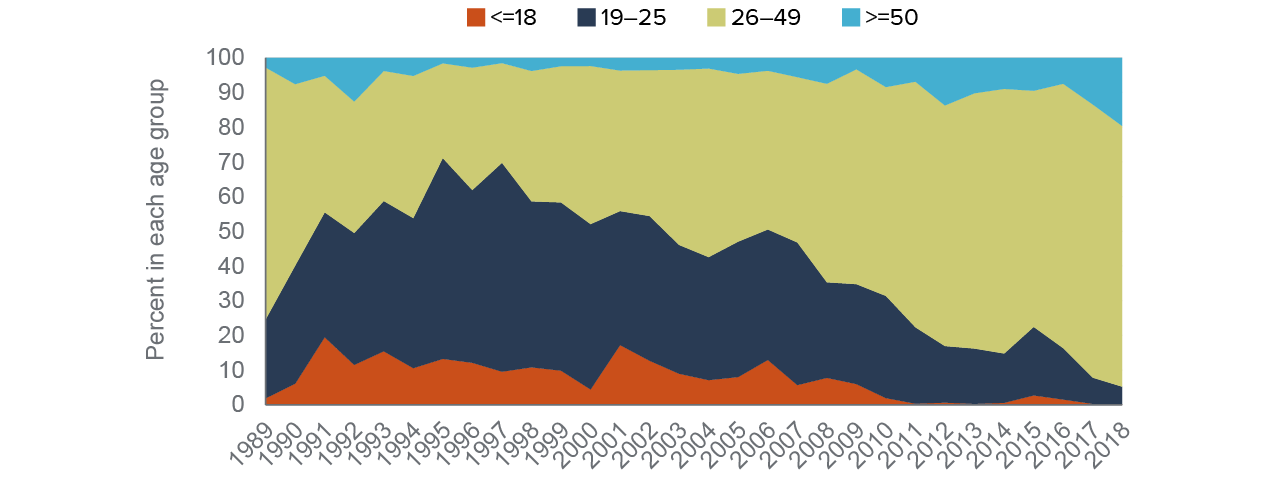
SOURCE: National Agricultural Workers Survey, fiscal years 1989–2018
NOTE: Weighted averages presented. Farmworkers include California survey participants, and immigrants are those born outside of the United States and Puerto Rico. Age groups coincide with the eligible ages for enacted or proposed Medi-Cal expansions. Undocumented status is self-reported.
The Governor Proposes a Further Expansion of Medi-Cal
Governor Newsom’s January 2022 budget includes a proposal to expand Medi-Cal eligibility to low-income adults ages 26–49, regardless of immigration status. If enacted, this would cover the last remaining age group of undocumented immigrants. The governor frames this change as a way to reach universal coverage, since undocumented immigrants make up the vast majority of the state’s uninsured population following the ACA.
The political climate seems hospitable to the idea of expanded coverage for undocumented Californians: 66 percent of adults support health care coverage for undocumented immigrants, according to the PPIC Statewide Survey (Baldassare et al. 2021). Figure 5 further demonstrates that most (75% in 2018) undocumented farmworkers fall into the 26–49 age category. In contrast, earlier expansions to children and young adults affected relatively small shares of these farmworkers.
Barriers to Health Care for Farmworkers
Although a wide range of barriers may affect farmworkers’ access to health care, the ability to pay deters many farmworkers from getting care. Cost is a key reason for missing health care or prescriptions among low-income immigrants, and among undocumented immigrants in particular (Cha and McConville 2021). Insurance defrays out-of-pocket payments; lack of insurance is more prevalent among undocumented immigrants and likely drives their cost concerns.
Cost or Lack of Insurance Is the Most Common Barrier
Among those who sought health care, cost and insurance dominate farmworkers’ descriptions of barriers to care. Thirty-five percent of undocumented farmworkers and 20 percent of documented farmworkers cite cost or lack of insurance as a barrier to getting care (Figure 6). In contrast, less than 10 percent of farmworkers report other barriers to care. These findings are similar to statewide patterns among low-income Latinos: delaying care due to cost or lack of insurance is a key barrier (62% vs. 38% reporting any other reason) (California Health Interview Survey 2019). Among uninsured low-income Latinos, the difference is starker (88% cost or lack of insurance vs. 12% reporting any other reason).
Barriers like transportation or not knowing where services are available are rarely mentioned as key difficulties in getting care even though farmworkers are likely to work in less urban areas than most immigrant workers in California. One expert from my interviews described contract farmworkers as sometimes working in multiple counties in a given week or month. Notably, undocumented status is infrequently cited, though immigration status clearly affects access to health insurance and the ability to pay for care.
Cost or lack of health insurance is by far farmworkers’ biggest barrier to health care
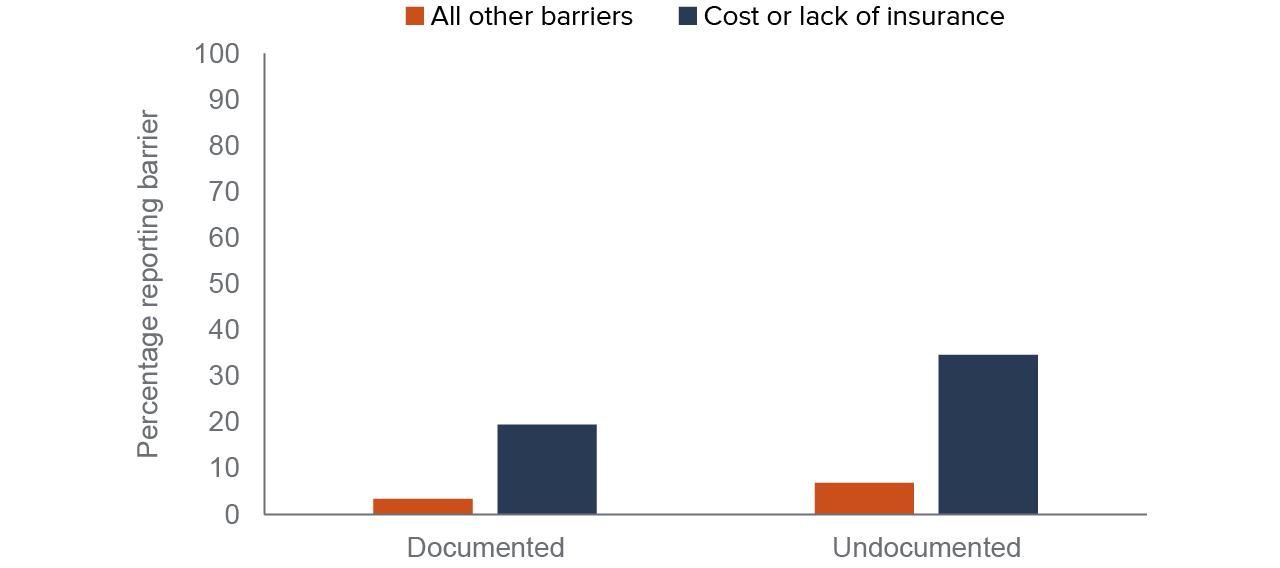
SOURCE: National Agricultural Workers Survey, fiscal years 2010–2017
NOTES: Weighted averages presented. Farmworkers include California survey participants, and immigrants are those born outside of the United States and Puerto Rico. Excludes farmworkers who report never needing health care in the US (8% of documented, 18% of undocumented). Undocumented status is self-reported. Farmworkers can report more than one barrier. “All other barriers” include undocumented status, no transportation or health provider too far away, not knowing where services are available, needed services not being available, health provider not open when needed, health provider not speaking the farmworker’s language, health provider not being respectful or welcoming, health provider not understanding the farmworker’s problems, and a fear of job loss due to seeking care.
Over half of farmworkers have low incomes (below 200% of the federal poverty level), with higher poverty rates among undocumented farmworkers. Although the average farmworker has income around 317 percent of federal poverty, workers with children—and especially undocumented workers with children—have lower incomes (215% and 200% of federal poverty on average). Median incomes are lower than the average; the median farmworker has an income equivalent to 191 percent of federal poverty.
Due to high poverty and high uninsured rates, Medi-Cal could serve this group well if eligibility were not a hurdle. Undocumented adults over age 26 primarily have access only to emergency and pregnancy-related services (Cha and McConville 2021). Most undocumented immigrants are ineligible for Medi-Cal and Covered California plans. They are, however, eligible for employer health insurance coverage, which is the most common form of coverage for Californians with insurance (Cha and McConville 2020).
Health Services Used by Farmworkers
Farmworkers have fewer health care options compared to immigrants in urban areas, especially if they lack legal immigration status. My colleague and I have detailed the health services landscape for California’s undocumented immigrants (Cha and McConville 2021). The providers and programs we profiled—community clinics, public hospitals, and county programs for the medically indigent—are important for the farmworker population as well, although reception to undocumented immigrants could be less welcoming in some agricultural areas. Los Angeles County, which has the largest number of undocumented immigrants in the state (Dietz et al. 2021), operates My Health LA, a health services program serving low-income undocumented patients. In contrast, some counties with large agricultural sectors—such as Tulare and Merced—exclude undocumented immigrants from their indigent care programs (Insure the Uninsured Project 2019).
Undocumented farmworkers were less likely than their documented counterparts to use either US-based or foreign health care. When workers had health insurance, however, it raised health care use by about 22 percent (Luo and Escalante 2018). In our survey data, most farmworkers report accessing health care in the past two years—in the US, abroad, or both—but undocumented workers are less likely to have gotten care in either of the locations (Figure 7). The higher rate of undocumented farmworkers reporting no care (44% vs. 23% of documented farmworkers) is consistent with research showing that undocumented immigrants in California are less likely to report having a usual source of care than documented immigrants (Cha and McConville 2021).
Most farmworkers report getting health care in the past two years
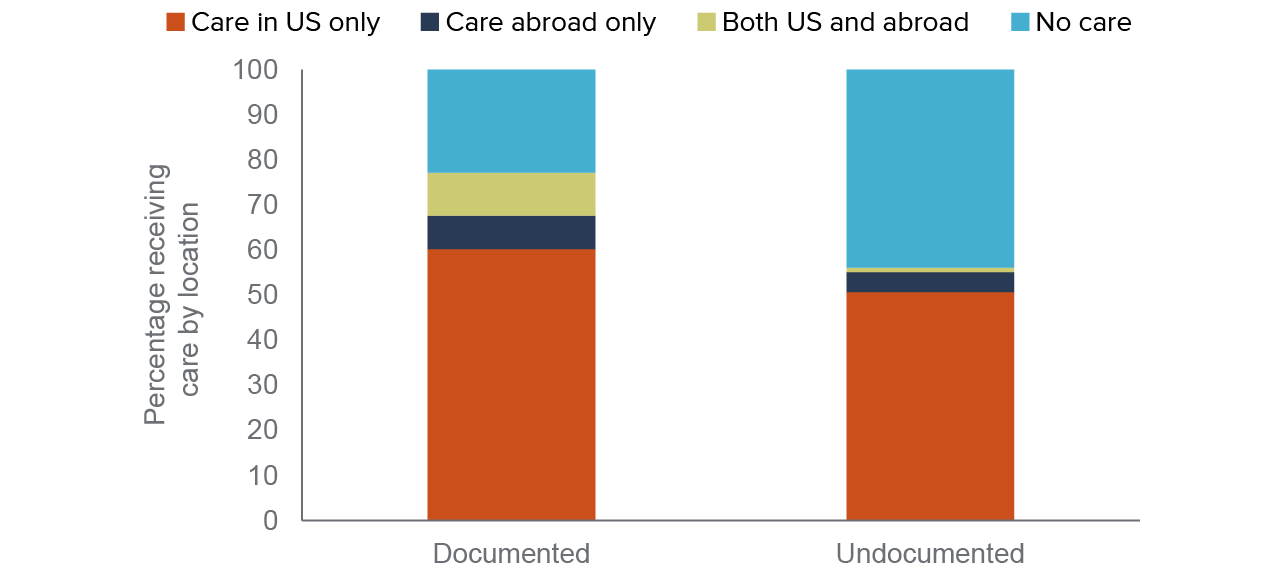
SOURCE: National Agricultural Workers Survey, fiscal years 2010–2017
NOTE: Weighted averages presented. Farmworkers include California survey participants, and immigrants are those born outside of the United States and Puerto Rico. Undocumented status is self-reported.
Clinics are Important Health Care Providers for Farmworkers
Among farmworkers who received health care in the US, the majority relied on clinics, with documented workers more likely to visit a doctor’s office and undocumented workers more likely to visit a public clinic (Figure 8); this aligns with past work finding that undocumented immigrants had access to proximate clinics (Lee, Hill, and McConville 2012). It also fits with findings that clinics are key health care access points for low-income immigrants in California (Cha and McConville 2021).
Most farmworkers getting care in the US rely on public clinics and doctor’s offices, not hospitals or ERs
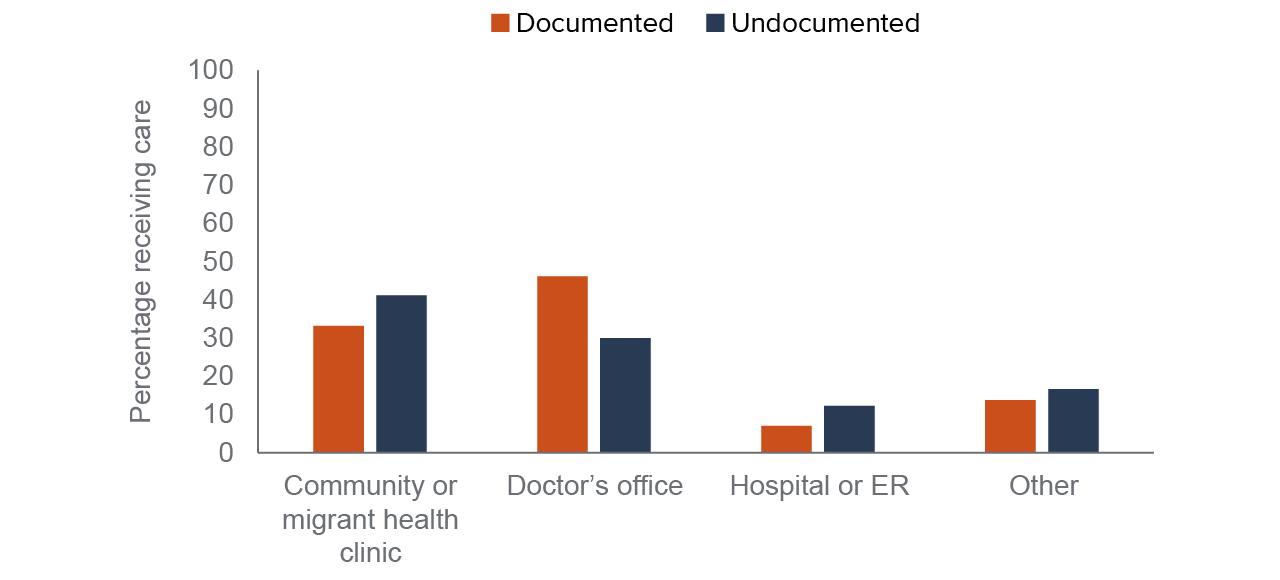
SOURCE: National Agricultural Workers Survey, fiscal years 2010–2017
NOTES: Weighted averages presented. Farmworkers include California survey participants, and immigrants are those born outside of the United States and Puerto Rico. Includes farmworkers who received health care in the US in the past two years of any type. Undocumented status is self-reported. Categories represent the location where farmworkers last received care in the US. “Doctor’s office” includes private clinics, and “other” includes healer/curandero, chiropractor or naturopath, dentist, and “don’t know.”
Employers Play a Significant Role in Farmworker Health Care
Growers and contractors in farm work have a long history of wanting to provide health insurance to their employees, according to experts interviewed for this study. In contrast to industries like food service and construction, which also have heavily immigrant workforces with significant numbers of undocumented workers, these experts indicated that produce growers have a history of providing health insurance or services to their employees.
Growers and contractors want their workers to be healthy and to recognize the benefits of staying with their employer. One expert expressed that providing health insurance helps to define the relationship between employers and employees. Employers are motivated to build this bond because of a tight farm labor market, combined with highly mobile and smartphone-savvy farmworkers, who have good information about employer quality.
One model of insurance described in interviews is for a membership organization to pool risk across many growers and contractors; the organization issues health insurance plans in the same way many large corporations cover their employees. The membership organization can then coordinate activities such as meeting workers in the field to discuss benefits, encouraging preventive care, and scheduling appointments with specialists. This wrap-around approach has been around for decades, but whether more employers have extended health care or services to farmworkers after the ACA employer mandate is unclear.
Some large agricultural employers offer direct health services rather than health insurance, which farmworkers may report in the NAWS as a community or private clinic, depending on their interpretation. An expert I spoke with explained that in specialty crops, growers try to directly hire the same workers year after year for their crop-specific skills. In the case of berries, the fruits ripen unevenly over time, and need repeated passes to harvest. Farmworkers remain with the crop for an extended period. Recruiting and retaining a skilled workforce is therefore a high priority, and berry growers may offer benefits like health services to compete for the best workers. Other experts emphasized that these motivations are not crop-specific, saying that the desire to give farmworkers health benefits is universal across the produce sector.
While the details differed, a wide range of interviewees with different perspectives emphasized the role of employers in farmworker health care. The analyses presented in the next section do not suggest that employer insurance changed following the ACA, so it may be that some employers were, and remain, committed to providing health care benefits, while others do not take this on.
Insurance Coverage Patterns after Policy Changes
Overall, health care insurance increased for undocumented farmworkers but more so for documented farmworkers. Medi-Cal coverage in particular increased for documented farmworkers after the expansion in California, but the changes associated with the employer mandate were muted or overtaken by Medi-Cal enrollments.
Increased Rates of Farmworker Insurance Reflect the Medi-Cal Expansion
Except for fiscal year 2010, insurance coverage among documented farmworkers increased over time, then leveled off in 2016. (Technical Appendix Table A3 shows that statistically adjusted analyses provide similar conclusions.) Figure 9 shows the changes in insurance coverage, Medi-Cal, and employer insurance for documented farmworkers. In the analyses, the increased insurance coverage grows to a maximum of 34 percentage points, or a 71 percent increase, in fiscal year 2016, before coming down somewhat in the last years of the study.
The increase in Medi-Cal follows a similar path. Over the study period, there is no clear pattern of employer insurance coverage over time: fiscal years 2013 and 2017 have the highest rates of employer coverage among documented farmworkers, suggesting no clear effect of the ACA employer mandate on coverage for this group.
Insured rates for documented farmworkers rose along with Medi-Cal coverage
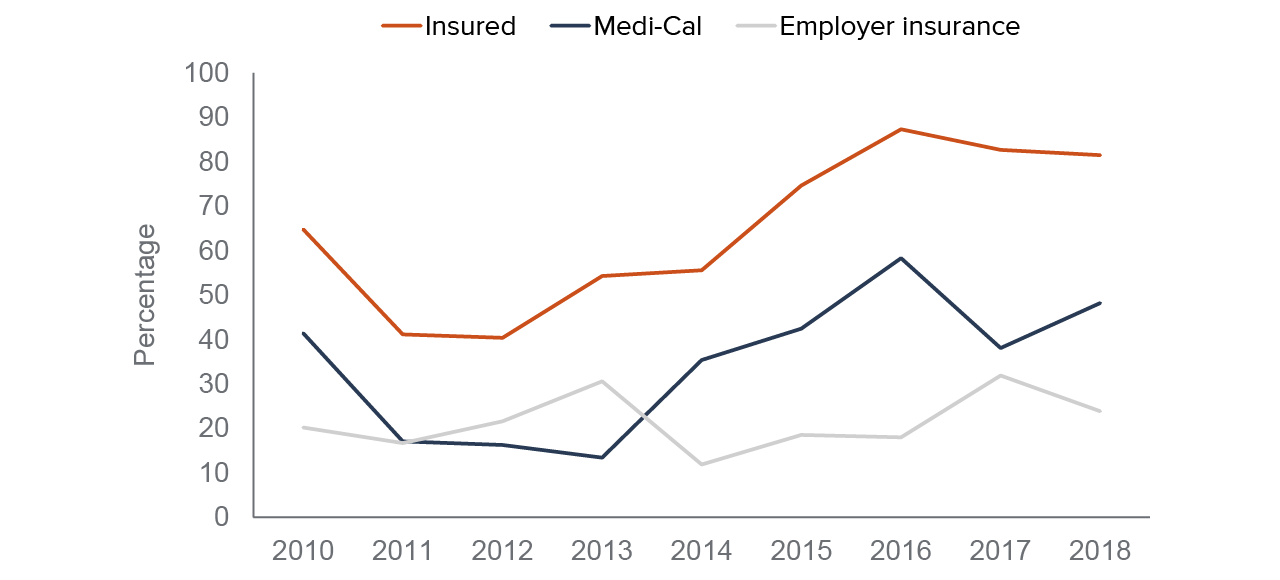
SOURCE: National Agricultural Workers Survey, fiscal years 2010–2018
NOTE: Weighted averages presented. Farmworkers include California survey participants born outside of the United States and Puerto Rico. Undocumented status is self-reported.
Not surprisingly, findings for undocumented farmworkers are quite different. Figure 10 shows the changes in insurance coverage, Medi-Cal, and employer insurance for undocumented farmworkers. Their insured rate is lower in the years following the ACA Medi-Cal expansion and the rollout of the employer mandate. Medi-Cal coverage and employer insurance both fluctuate over time, but not in ways systematically correlated with health insurance policy changes. The increase in Medi-Cal coverage around 2014 is likely to be the emergency version of the program, but this change is much smaller than for documented farmworkers. In adjusted analyses, undocumented farmworkers’ insurance coverage was the highest in 2011, 2012, and 2013, years that preceded the health insurance policy expansions covered in the study period (Technical Appendix Table 3). Reported Medi-Cal coverage in particular was highest in fiscal year 2013 among undocumented farmworkers, and it is lower in the post-ACA-expansion period.
Neither Medi-Cal expansion nor the employer mandate correlated with large insurance gains for undocumented farmworkers
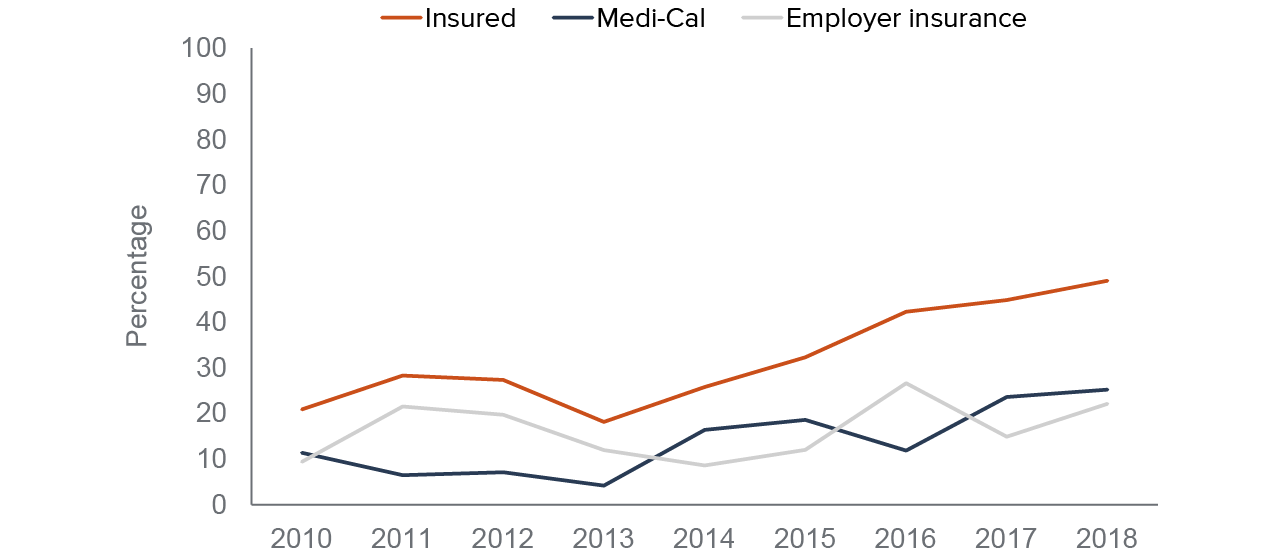
SOURCE: National Agricultural Workers Survey, fiscal years 2010–2018
NOTE: Weighted averages presented. Farmworkers include California survey participants born outside of the United States and Puerto Rico. Medi-Cal is the author’s interpretation of government payment for health insurance reported by workers. Undocumented status is self-reported.
These patterns suggest that changes to undocumented workers’ sources of coverage did not correlate to policy changes—and in particular the employer mandate to offer insurance. The reported rates of Medi-Cal are likely to be restricted-scope care, or health services for specific covered conditions, which became available with the ACA expansion. There was also no discernable increase in coverage following the SB 75 expansion to young adults in 2016, which may simply reflect the relatively small statewide numbers of undocumented young adult farmworkers relative to older undocumented farmworkers (Figure 5, earlier).
The Employer Mandate Was not Associated with More Employer Coverage
As noted above, the findings for employer-supplied coverage differ quite a bit from the Medi-Cal results. Farmworkers’ own employer insurance changed over time in ways uncorrelated to the employer mandate rollout (Figure 9 and Figure 10, earlier). Farmworkers’ coverage through employers actually declined after the employer mandate was introduced (see Technical Appendix Table A3 for statistically adjusted analyses), while coverage for undocumented farmworkers fluctuated in ways inconsistent with the policy timing. For both of these groups, it seems that the employer mandate was not likely to have made a meaningful difference in their access to health insurance—or, by extension, reduction of cost barriers to care.
According to one expert, some employers who had offered health insurance to farmworkers before the ACA experienced “crowd-out” due to the Medi-Cal expansion. Crowd-out describes when individuals switch from private insurance to public insurance as a result of new eligibility for public coverage.
While employer coverage has out-of-pocket costs like premiums and co-pays, Medi-Cal requires zero cost-sharing from most of its enrollees. Levels of employer coverage may not have changed because, while more employer coverage was available, individuals opted for Medi-Cal instead. If crowd-out is characterized by younger, healthier workers switching to Medi-Cal, this could lead to higher costs for those remaining on employer insurance, since employer plans would be responsible for supporting an older, more expensive population.
Another possibility is that fewer employers fall under the ACA employer mandate than expected. Growers can hire farmworkers directly, acquire labor through contracting companies, or a combination of the two. According to an expert interviewed for this study, direct hire is more common when employers need labor over an extended period rather than, for example, concentrated in a brief harvest.
For growers, the number of workers hired depends on many factors, including the crop type. Growing and harvesting commodities such as almonds involves a lot of mechanization, reducing the number of farmworkers needed. As a result, very large operations can have fewer than 50 employees, which is the threshold for the ACA employer mandate. Mechanization also means that farmworkers are interchangeable and individual skill is less important, possibly reducing growers’ need to retain specific workers.
Farm labor contractors, or FLCs, act as intermediaries in the agricultural labor market. They have a strong presence in California’s agricultural industry; as of March 2021, there were over 5,000 registered FLCs based in California (US Department of Labor 2021). It is difficult to estimate of the size of FLC operations precisely, although over three-quarters of private employers in California agriculture and related industries have fewer than 50 employees (Figure 11). This suggests that FLCs will tend to fall well below the ACA employer mandate threshold.
The experts I spoke with described FLCs as highly variable in terms of size, professionalization, and treatment of their contract farmworkers. A Sonoma County study documented lower rates of health insurance among contract farmworkers compared to farmworkers hired directly, though their finding was not significant (Moore et al. 2016). The experts had a range of opinions on whether FLCs offer health coverage at similar rates to growers; some said FLCs and growers are equally concerned with farmworker health care access, while others argued that growers tend to offer more benefits than FLCs.
Most private employers in agriculture and related industries do not need to comply with the employer health insurance mandate
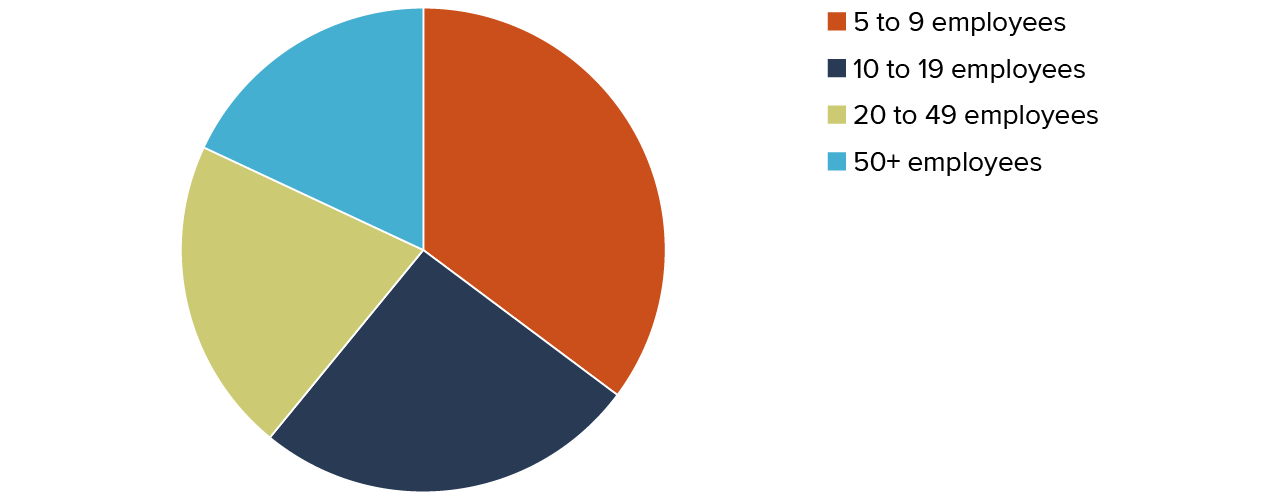
SOURCE: First quarter 2020, US Bureau of Labor Statistics 2022
NOTE: Includes private establishments in California that fall under North American Industrial Classification System (NAICS) code 11 (agriculture, forestry, fishing, and hunting sectors). These estimates exclude establishments that do not have full employment and wage data publicly available on the Bureau of Labor Statistics site. The Affordable Care Act’s employer mandate applies to businesses with 50 or more employees.
Seasonal work patterns and the increasing prevalence of contract labor and greater mechanization may mean that, despite being a $50 billion industry, most agricultural employers simply are not required by the ACA to extend insurance options to the workers in their fields, orchards, and vineyards. Even documented farmworkers, who can get full-scope Medi-Cal (if they meet income criteria) or purchase private coverage on Covered California, only had an 82 percent insured rate in fiscal year 2018, meaning that nearly one-fifth lack coverage.
Despite large policy changes in recent years, the need for affordable coverage, whether through employers, public insurance, or the marketplace, remains high for farmworkers. Identifying options for those who fall between the gaps will be a focus for policymakers, including the Healthy California for All Commission, which is charged with the task of planning a unified financing system that covers all Californians (California Health and Human Services Agency 2021). The ongoing COVID-19 pandemic raises the stakes of addressing health insurance and health care barriers for farmworkers, considering that agricultural work continues despite the health risks.
Fewer Cost or Insurance Concerns for Documented Immigrants
Undocumented farmworkers report cost or lack of insurance as a barrier to care at higher rates than do documented farmworkers. Cost concerns have, however, fluctuated over time for documented and undocumented farmworkers when controlling for other variables (Technical Appendix Table A4).
In fiscal year 2016, the year when insurance rates and Medi-Cal coverage peaked for documented workers, concerns about cost were significantly lower, although the other years following Medi-Cal expansion are similar to fiscal year 2013. For undocumented workers, cost as a barrier did not decline after the ACA policy changes. In fact, cost was a greater concern in some of the post-expansion years. The differences between the two groups’ reporting of cost barriers were significant in almost every year.
The timing of health insurance policies does not appear to be associated with changes to cost barriers for direct or contract employees. This is not surprising because there is no evidence that farmworkers who are hired directly or who are contracted workers were more likely to benefit from employer insurance following the employer mandate rollout (Appendix Table A7).
Conclusion and Recommendations
After recent health policy changes, what has changed for health insurance and barriers to care for farmworkers? Changes have not always come in expected ways, and changes have been unevenly distributed across farmworkers. The ACA employer mandate was not associated with increased insurance rates in general, nor with increased employer coverage in particular. However, the ACA Medi-Cal expansion did correlate with increased insurance and Medi-Cal coverage, but only among documented farmworkers. After the expansion, there is some evidence that fewer of these workers experienced cost or lack of insurance as a barrier to care.
Although I heard from some experts that farmworkers hired directly have better benefits than those hired through farm labor contractors, this did not manifest as employer insurance coverage. Insurance coverage for direct hires did not increase when the employer mandate was rolled out. It is possible that increased mechanization in agriculture has resulted in few companies with 50 or more workers, the threshold for the employer mandate. It is also possible that the Medi-Cal expansion produced crowd-out (in which people turn down private insurance to enroll in public insurance), eroding some amount of employer coverage expansion.
As California works towards a unified financing system for health care, most farmworkers will likely fall under some form of coverage. The question of whether and how to extend coverage and care to the largest group of undocumented immigrants—ages 26 to 49—is unanswered, but the state is discussing proposals. The governor’s budget includes a proposed expansion to this group in 2024. One expert raised the questions of how health care could be unified over time and what role employer coverage may play in the future. Crowd-out to Medi-Cal can worsen the insurance risk pool, threatening the affordability (and even viability) of employer coverage of farmworkers.
Undocumented farmworkers could gain access to insurance by having their status regularized through federal reform, though this is not likely to happen soon. President Biden’s vision for immigration reform includes paths to citizenship for undocumented immigrants and fast-track regularization of status for undocumented farmworkers. A previous federal proposal called AgJOBS included a similar provision, but the policy was never enacted (Martin and Taylor 2013).
Although the discussion of farmworkers aging and settling presented these changes as a source of vulnerability, interviewees saw the presence of family in the US as a strength. Family members can help promote health. One barrier to understanding health information is lower education; involving farmworkers’ children and spouses in medical visits and treatment plans can increase health literacy by making the process collaborative. Family members can also be part of treatment plans, such as new exercise routines.
I also learned that public health efforts could deploy a family-based approach during the pandemic. Disseminating COVID-19 vaccination information through family channels may be more culturally appropriate than social media campaigns. Trusted nonprofit and educational groups, including legal services organizations, schools, and migrant education programs, can play roles in sharing public health information. Vaccine clinics that inoculate farmworkers and their family members can control coronavirus spread through farmworker communities more effectively than those focusing only on workers.
State policy changes under discussion are likely to benefit farmworkers’ access to insurance coverage care, but challenges will remain. An adequate supply of farmworkers is one challenge. It is not clear whether new coverage options for undocumented immigrants will increase the farm labor supply by drawing workers from other agricultural destinations. In the past, farmworkers tended to migrate to places where they have personal networks rather than being attracted by generous safety nets (Pena 2009; 2014).
Another, equally complex problem is the lack of affordable housing options for farmworkers. Crowded housing is a key factor for health in this time of COVID-19. Given farmworkers’ important role in the economy and food supply chain, protecting their health could benefit all Californians.
Topics
COVID-19 Health & Safety Net Immigrants in California PopulationLearn More

California’s Farmworkers and Their Children Are Vulnerable to Food Insecurity

Health Coverage and Care for Undocumented Immigrants: An Update

Health Risks Persist for Older Farmworkers as COVID Lingers

Policy Brief: Pandemic Changes to Medi-Cal and Implications for California’s Immigrant Farmworkers

Public Health Insurance in California

Storms, Floods, and COVID-19 Have Worsened Long-standing Farmworker Housing Challenges

Video: Health Care Access among California’s Farmworkers