Summary
In 2014, the first year of Affordable Care Act (ACA) implementation, the number of Californians with health insurance increased substantially. However, millions of state residents continue to lack comprehensive health coverage, and those who remain uninsured are likely more difficult to enroll through traditional strategies.
In this report, we find that uninsured rates are highest for young men and for those with low levels of education, income, and employment. The prevalence of these same characteristics among correctional populations suggests that the justice system-and, in particular, county jails-may offer points of contact for many uninsured individuals who would otherwise be hard to reach.
Outreach and enrollment efforts aimed at local jail populations are set within the policy context of California’s 2011 Public Safety Realignment, which created incentives and resources for local corrections agencies to improve reentry outcomes. With expansions in access to health insurance coverage under the ACA, nearly all counties are establishing programs to provide enrollment assistance to jail inmates as part of a more comprehensive reentry strategy. But resources and capacity are limited, so it is important to identify effective models to maximize the potential of county correctional systems as sites of insurance enrollment.
Introduction
California has made major strides in reducing the number of state residents who do not have health insurance. The state’s implementation of the Affordable Care Act (ACA) in 2014 expanded public insurance coverage through Medi-Cal, the state’s Medicaid program, and provided new options for federally subsidized insurance coverage through Covered California, the state’s insurance marketplace. Still, more than 4 million Californians continued to lack comprehensive health coverage in 2014-even after sizeable investments in public information campaigns, outreach activities, and enrollment assistance in the lead-up to and first year of ACA implementation. Although more recent estimates suggest further declines in California’s uninsured rate in 2015, between 3.25 million and 3.85 million Californians remain without health coverage.1 Those who continue to lack insurance are likely to be more difficult to reach and enroll.
To address this difficulty, the state passed legislation that allocates nearly $25 million for enrollment efforts focused on special population groups. The funding goes to local community organizations and county agencies to provide focused enrollment assistance for several groups-including people with mental health or substance use issues, homeless individuals, young men of color, and people under state and county correctional authority. In addition, a 2013 state law that facilitates enrollment assistance within jails has removed many barriers to enrolling correctional populations in California (Bird and McConville 2014).2
It is important to understand these enrollment efforts in the policy context of California’s Public Safety Realignment. Implemented in 2011, realignment shifted responsibility for the supervision of lower-level felons from the state to the counties. Although this major policy change was instigated by a court-mandated reduction in the state prison population, the realignment legislation also promoted the use of evidence-based reentry practices and advanced the notion that these practices can be more successful at the local level (Petersilia 2014; Bird and Grattet 2014). This shift toward local responsibility increased incentives for county justice systems to invest in reentry programming-coordinated services and supports designed to help former inmates transition back into the community and avoid further contact with the criminal justice system. Facilitating connections to health insurance coverage under the ACA could support these efforts.
In this report, we describe the characteristics of those who remain uninsured in California under the ACA. We compare these populations with correctional populations and use new information about California’s local jail population to assess the potential of county jails to enroll those who continue to lack health coverage. We conclude with a discussion of key design and implementation decisions county jails face in creating and sustaining health care enrollment assistance programs.
Who Is Still Uninsured in California?
In the first year of ACA coverage expansions, the percentage of Californians without health insurance dropped from 17.2 percent in 2013 to 12.4 percent in 2014-representing an increase of nearly 2 million residents with health coverage. Nonetheless, more than 4 million California residents were without comprehensive health insurance in 2014. Undocumented immigrants, who are largely excluded from the coverage expansions under the ACA, comprise a large share of this group: available estimates suggest nearly one million uninsured residents in California in 2014 were not eligible for financial assistance due to their immigration status. But more than 2 million California residents who are eligible for free or subsidized coverage remain uninsured (Garfield et al. 2016).
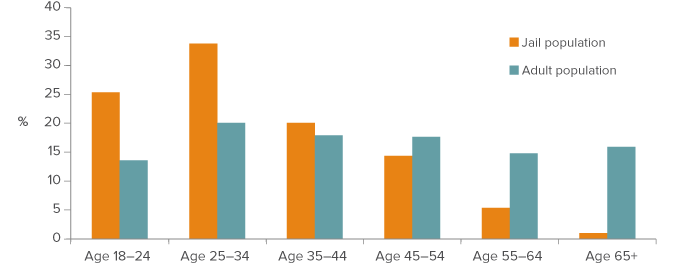
What do we know about those who continue to lack health insurance? Nearly six in ten uninsured California adults are men and about seven in ten are between the ages of 18 and 44. In fact, men under age 45 are overrepresented among the uninsured: they make up 35 percent of Californians who were uninsured in 2014, but only about 19 percent of the state’s general population. The overall age distribution of the uninsured skews heavily toward young adults, with people age 25 to 34 comprising the largest share of those without coverage. They are also the most overrepresented among the uninsured relative to their share of the California adult population (Figure 1).
Figure 1. Young adults are disproportionately represented among remaining uninsured
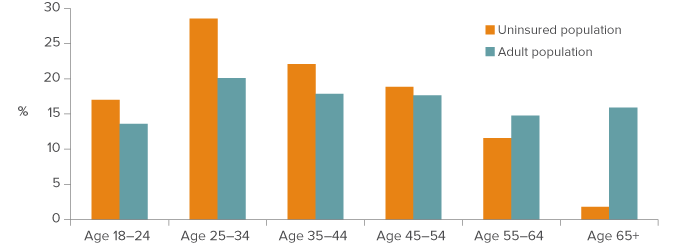
SOURCE: 2014 American Community Survey, Public Use Microdata Sample.
NOTE: Includes all California adults age 18 and over.
Adults with low education levels, low family incomes, and unstable employment are also disproportionately likely to be uninsured-even though the shares without insurance have declined significantly, uninsured rates in these groups remain stubbornly high. Among adults who did not finish high school, 35 percent were uninsured in 2014, down from nearly 45 percent one year earlier. Similarly, more than 30 percent of unemployed adults and those with family incomes below 138 percent of the federal poverty level (FPL)—the income eligibility threshold for the Medi-Cal program-continued to lack coverage, despite also experiencing a 10 percentage point drop in uninsured rates during this period. Uninsured rates are even higher for young males who have low education levels and are not steadily employed. Nearly 45 percent of men age 18 to 44 who did not graduate from high school were uninsured in 2014, and 36 percent of unemployed men in this age group were uninsured.
Figure 2. Uninsured rates remain high for adults with low education and income levels and those seeking work
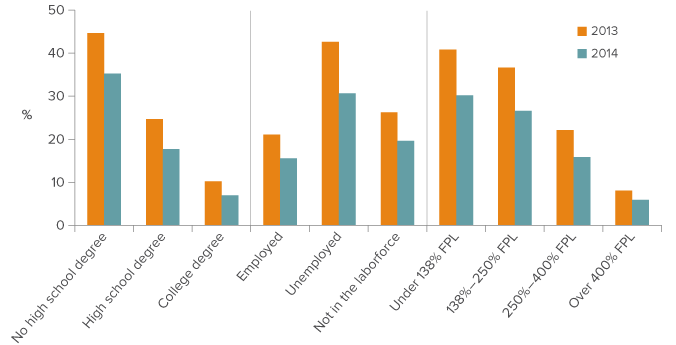
SOURCE: American Community Survey, Public Use Microdata Sample, 2013 and 2014.
NOTE: Insurance coverage is measured at the time of the survey. Results shown are for all California adults age 18-64. Income levels are presented as poverty rates based on federal poverty level (FPL) thresholds related to income eligibility cutoffs for health insurance coverage programs including Medi-Cal (under 138% FPL), premium and copayment subsidies available for coverage purchased through Covered California (138-250% FPL), and premium subsidies only for coverage purchased through Covered California (250-400% FPL).
The ACA is focused on helping people with low family incomes get health insurance, but about 70 percent of California adults who did not have insurance in 2014 had family income levels that should have qualified them either for free coverage through the Medi-Cal program or for heavily subsidized coverage through Covered California (technical appendix Table A1). It is conceivable that this high rate is being driven by California’s undocumented immigrant population, which-as we have already noted-is largely ineligible for coverage; this population tends to be younger and has higher shares of men and low education levels relative to the general population.
To assess this possibility, we examined the likelihood of being uninsured more closely.3 We found that young men remained significantly more likely to be uninsured in 2014 even after we control for undocumented status and a variety of other characteristics, including race/ethnicity, income level, education, employment, and marital status.
Figure 3 shows the predicted probabilities of men age 25 to 34 being uninsured across three levels of disadvantage, which are based on education, income, and employment levels. In the high disadvantage category-comprised of young men who did not finish high school, have incomes below 138 percent FPL, and are unemployed-the probability of being uninsured in 2014 is 64 percent for Latinos and about 50 percent for non-Hispanic whites and blacks. The likelihood of being uninsured is considerably lower at lower levels of disadvantage. For men age 25 to 34 with a high school education, incomes between 138 and 250 percent FPL, and current employment-in the medium disadvantage category-the likelihood of being uninsured is cut nearly in half but remains relatively high (about 25% to 38% across racial/ethnic groups). And for a younger man in the least disadvantaged category-comprised of those who have a college degree, incomes above 250 percent FPL, and current employment-the probability of being uninsured in 2014 is considerably lower (about 13% for Latinos and about 8% for whites and African Americans).
Figure 3. Among young men, high levels of disadvantage point to a high probability of being uninsured
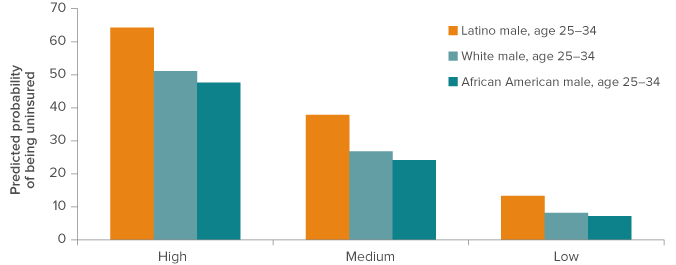
SOURCE: 2014 American Community Survey, Public Use Microdata Sample.
NOTE: Predicted probabilities are calculated based on the results of logistic regression analysis modeling the likelihood of uninsured status in 2014. In addition to sex, age, and the markers of disadvantage (education, poverty level, and employment status), the model also includes controls for undocumented status and marital status. All results in the figure are for individuals who are not flagged as undocumented and have never been married.
There are many reasons why people may not enroll in available coverage options, including affordability, personal preference, and a limited understanding of the role of health insurance. Others may lack resources or access to people or institutions with information about available coverage and the ability to assist with enrollment. Adults who have had contact with the criminal justice system are especially likely to have limited contact with traditional connections to health insurance coverage, such as higher education institutions or employers; they may also lack community ties that could provide information on low-cost coverage options.
It is important to recognize that many of the characteristics prevalent among the uninsured-including low education levels and unemployment-have been linked to a higher likelihood of being involved with the criminal justice system (Gould et al. 2002; Lochner and Moretti 2004). Moreover, there may be considerable overlap between Californians who have contact with correctional institutions and the groups of Californians who continue to have high uninsured rates. Nationwide, nearly three in four adults housed in correctional institutions-including inmates in state, county, and federal correctional facilities-are between the ages of 18 and 44, and more than nine in ten are male. Incarcerated adults have low education levels relative to the general adult population; more than 30 percent have not graduated from high school and fewer than 5 percent have college degrees. Very few are married, and the share with disabilities is very high: one in four report at least one disability that affects basic functioning (technical appendix Table A3). For these reasons, targeting correctional populations for enrollment outreach could play an important role in reducing the number of uninsured Californians.
County Jails as Sites of Enrollment
California’s jails may prove particularly promising sites to target enrollment assistance due to the high volume of individuals with whom they have contact. In 2014, the county jail system had an average daily population of about 80,000 inmates.4 It is difficult to pinpoint the actual number of inmates, given the significant amount of turnover in local jails. Nationwide, there were more than 11.4 million admissions to local jails in 2014, roughly 15 times the average daily population (Minton and Zeng 2015). When we apply this ratio to California’s system, we estimate that jails had more than 1.1 million admissions in 2014.5 And available evidence suggests that many of those with jail contact are uninsured and eligible for Medi-Cal (Bandara et al. 2015; Somers et al. 2014).
Information on the size and characteristics of California’s jail population has historically been quite limited. However, a new data collection effort initiated in response to realignment has begun to fill these informational gaps. The BSCC-PPIC Multi-County Study (MCS) is a collaborative effort between the Public Policy Institute of California (PPIC) and the California Board of State and Community Corrections (BSCC) to work with a representative group of 12 counties to capture in-depth, individual-level data on their correctional populations. The participating counties are Alameda, Contra Costa, Fresno, Humboldt, Kern, Los Angeles, Orange, Sacramento, San Bernardino, San Francisco, Shasta, and Stanislaus. This group of counties, comprising about two-thirds of the total population, reflects the demographic composition and regional distribution of the statewide population. Nonetheless, characteristics of the population in other local jurisdictions may be different.
We estimate an average daily population of about 55,000 inmates in 2014 for the county jail systems included in this study.6 We find that approximately 455,000 adults, or more than eight times the average daily population, had contact with these county jail systems at some point over the course of the year.7 Nearly three-quarters (72%) of these individuals were booked only once, while a small group-about 14,000 individuals-had five or more jail contacts over the one-year period.
These individual-level jail data indicate that jail inmates in California tend to be younger than the general population. Figure 4 compares the age distribution of the jail population to that of the general adult population for the counties under study. Interestingly, the comparison shown in Figure 4 is similar to the age distribution of the uninsured relative to the general population shown in Figure 1.
Figure 4. Young adults are overrepresented in California’s jail population
SOURCE: MCS data, 2014; 2014 American Community Survey, Public Use Microdata Sample.
NOTE: The age profile of the jail population is based on the characteristics of adults moving through the jails systems of the study counties. The general adult population represents Californians age 18 and older in the study counties.
Unsurprisingly, we find that the vast majority (77%) of adults moving through the jail system are men-this gender difference holds across local, state, and federal justice systems. We also observe that Latinos and, in particular, African Americans are overrepresented among adults with jail contact. Figure 5 summarizes the gender and racial/ethnic composition of this population.
Figure 5. California’s jail population is disproportionately male and non-white
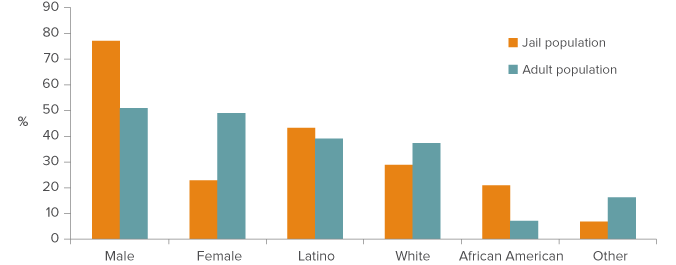
SOURCES: MCS data, 2014; 2014 American Community Survey, Public Use Microdata Sample.
NOTES: Jail population estimates are based on the characteristics of adults moving through the jail system in the counties under study. Adult population estimates include Californians age 18 and older in the counties under study.
The jail population is likely to be difficult to reach via traditional sites, such as employment or educational institutions. But, given the demographic similarities between California’s jail population and its uninsured population, outreach efforts within jail systems have the potential to help the state meet its goal of expanding health coverage.
There is evidence that insurance enrollment improves health outcomes for former inmates and that it may reduce recidivism.
Enrollment outreach in jail systems may also have benefits beyond improving health insurance coverage. There is evidence that insurance enrollment improves health outcomes for former inmates and that it may reduce recidivism (Freudenberg et al. 2005; Morrissey et al. 2007; Mancuso and Felver 2009). Specifically, chemical dependency treatment and outpatient mental health programs have been associated with reductions in rearrests and fewer total arrests (Morrissey et al. 2006; Mancuso and Felver 2009). These findings predate the ACA and are limited to inmates eligible for Medicaid-and, of course, insurance coverage alone does not guarantee an increase in the use of health services. But higher treatment rates among ex-offenders with severe mental illness and substance use disorders were reported for former inmates when they had Medicaid coverage (Morrissey et al. 2006; Shah et al. 2013).
Several changes underway within the Medi-Cal program suggest that enrollment could prove even more beneficial than in the past. Efforts to better integrate mental and physical health services, an overhaul of the Drug Medi-Cal program that provides treatment for substance use disorders, and the development of pilot projects that connect Medi-Cal beneficiaries to social services-including housing and case management-could all prove especially salutary to those under the supervision of county correctional systems.
Designing Enrollment Assistance Programs
Opportunities for increased insurance coverage created by recent state and federal policy changes rely heavily on effective local implementation. Under realignment, county correctional systems face stronger incentives to invest in reentry assistance and many local corrections and health practitioners recognize the benefits of expanded access to health coverage and care. Although increased responsibilities under realignment and limited resources can make it difficult to prioritize health insurance enrollment assistance for this population, most counties report that they are providing some form of assistance for individuals under correctional supervision (Californians for Safety and Justice 2015). As counties continue to develop and implement enrollment assistance programs, it will be important to understand whether the decisions they make help them meet their goals-goals that may vary across counties, and even across agencies within the same county.
Counties are covering the cost of these programs in a variety of ways, including using public safety realignment funds, county general funds, and state and federal Medi-Cal administrative funds. There are also differences in the relationships between county jail systems and other entities that can provide enrollment assistance-especially county welfare departments, the county agencies responsible for administering Medi-Cal enrollment. In many cases, realignment has forged or strengthened these relationships by requiring the counties to create Community Correction Partnerships (CCPs) that are tasked with the implementation and management of realignment within each county. In recognition of the need for a holistic approach to reentry, these CCPs include representatives from county correctional and court systems and also from county social services and health agencies. Through CCPs, counties can bring often siloed agencies together to connect correctional populations to services and supports that could reduce recidivism. CCPs also create opportunities to coordinate goals, strategies, and funding.
The degree of coordination across county agencies and the types of funding available to support enrollment efforts have implications for program scope and sustainability. Highly coordinated counties may be able to leverage expertise and points of contact across agencies to accomplish more with fewer resources. In resource-constrained environments, however, collaborators may need to choose between enrolling as many uninsured individuals as possible and offering enrollment assistance to specific high-need populations. And if counties opt to focus on high-need groups, they will need to decide how to target those efforts. Health and human services agencies may focus on those with high general health needs, while corrections agencies may focus on high behavioral health needs that are related to greater involvement with the criminal justice system. Similarly, health and human services agencies may prioritize individuals who drive up county health costs with their frequent emergency room contact, while correctional agencies may target individuals who drive up correctional health care costs through hospital stays while in custody. Realizing the potential gains from coordination and collaboration across agencies requires a program model that balances the goals of different stakeholders.
Counties may also need to confront trade-offs between the size of the population targeted for intervention and the intensity of the treatment provided. Although the implementation process is still in its early stages, two primary methods are emerging for identifying groups within the jail system in need of enrollment assistance. The first focuses efforts on the relatively broad population flowing into jails; the second concentrates on convicted jail inmates nearing the end of their terms.
The first approach, which we refer to as the “front door” strategy, targets all individuals who are booked into jail on a new arrest, warrant, hold, or supervision violation, as well as those committed to jail to serve sentences. This model uses the booking process as an opportunity to screen for health insurance coverage and to provide targeted assistance to the uninsured. In the counties included in the MCS study, the front-door group would include all 455,000 individual adults who were booked into county jails at some point in 2014. Nearly 30 percent were admitted and released on the same day, while another 45 percent spent less than two weeks in custody (Figure 6).
A second approach, which we refer to as the “back door” strategy, focuses efforts on a narrower population of individuals who were convicted of offenses, received jail sentences, and are nearing the completion of those sentences. Enrollment assistance can be provided to this population as part of a comprehensive reentry planning strategy. In our data, about 70,000 adults were released back into the community in 2014 after serving jail sentences. Unsurprisingly, this back-door group spent more time in custody than the front-door group: about one-third served a continuous term of more than 60 days and another 18 percent served between one and two months. Given these longer periods in custody, the back-door model generally allows more time for substantial enrollment assistance, spanning from screening to assistance with applications to follow-up to confirm enrollment.
Figure 6. The back-door population spends more time in custody
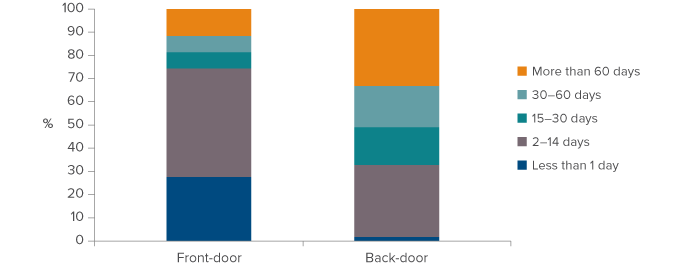
SOURCE: MCS data, 2014.
NOTE: Jail population estimates are based on adults moving through the jail system in the counties under study.
Under either strategy, enrollment assistance could range from providing basic information to more comprehensive assistance. However, the front-door strategy’s target population is more than six times the size of the population targeted by the back-door strategy, and this affects the level of resources that could be devoted to each individual. There are few differences in the demographic characteristics of the two groups, although individuals targeted after serving jail sentences are slightly more likely to be male and less likely to be Latino than those in the front-door group (technical appendix Table B1).
Looking Forward
California has made substantial progress in increasing insurance coverage under the ACA. In 2014, the number of uninsured residents declined by 2 million, nearly 5 percentage points. However, millions of residents remain uninsured, and state and local agencies continue to try to connect those who are eligible to available coverage options. We find that uninsured Californians in 2014 are disproportionately young and male. Among young men, we find that those with low education levels, low incomes, and less attachment to employment are especially likely to be uninsured.
California’s jail system may offer important opportunities to reach a share of the uninsured-particularly those who are harder to reach through traditional enrollment mechanisms. In addition to helping the state meet its health insurance coverage goals, enrollment assistance efforts offer the potential to leverage federal and state Medi-Cal resources to improve access to needed physical and behavioral health resources for the reentry population. Existing research suggests that interventions that improve access to health-related services could go a long way toward reducing recidivism, and the associated cost savings have the potential both to reduce the correctional cost burden on counties and to free up resources for additional reentry programming. As counties initiate and expand enrollment assistance efforts, the diversity in their approaches can help us track key differences among models and identify best practices.
Topics
Criminal Justice Health & Safety Net