

Financing Medi-Cal, California’s Medicaid program, has strained the state budget in recent years, despite the federal government covering a large majority of costs. One strategy to reduce the state’s financial commitments to Medi-Cal is to lower enrollment, but a larger uninsured population due to state and federal changes could prove costly in other ways.
In recent years, California has expanded Medi-Cal eligibility to low-income residents regardless of immigration status—together with pandemic-related growth, the expansion has contributed to high enrollment. Medi-Cal now covers more than 14 million Californians, over a third of the state’s residents. This high enrollment, coupled with higher-than-expected costs for the average participant, has increased Medi-Cal’s costs. (However, underlying mechanisms related to managed care and covering undocumented enrollees are not fully understood.)
Undocumented adults enrolled in Medi-Cal in larger numbers than expected and may have needed more substantial care. In 2025, California borrowed $3.4 billion and imposed cost-cutting policies to address Medi-Cal’s growth, including a freeze on new undocumented adult enrollment. Also last year, the passage of the federal HR 1 bill included significant changes that will further affect eligibility, enrollment, and federal financial contributions to Medi-Cal.
One consequential federal change is the introduction of work requirements for many adults. Beginning in 2027, Medi-Cal will require certain adults to work or meet community engagement criteria to receive benefits, although for the first 12 months people are allowed to self-attest. A new state policy will mirror these requirements for adult undocumented participants.
The state’s Legislative Analyst’s Office estimated that work requirements alone would lead 1 million people to exit Medi-Cal. Recent federal updates may interpret work exemptions for health reasons strictly, which also may increase disenrollments. These federal changes will coincide with California’s efforts to shrink the state’s Medi-Cal budget.
Reducing undocumented participants by freezing enrollment is a major step for California, as the state pays for almost all their program costs. Indeed, undocumented adult enrollments have declined by 6% since January, when the freeze began.
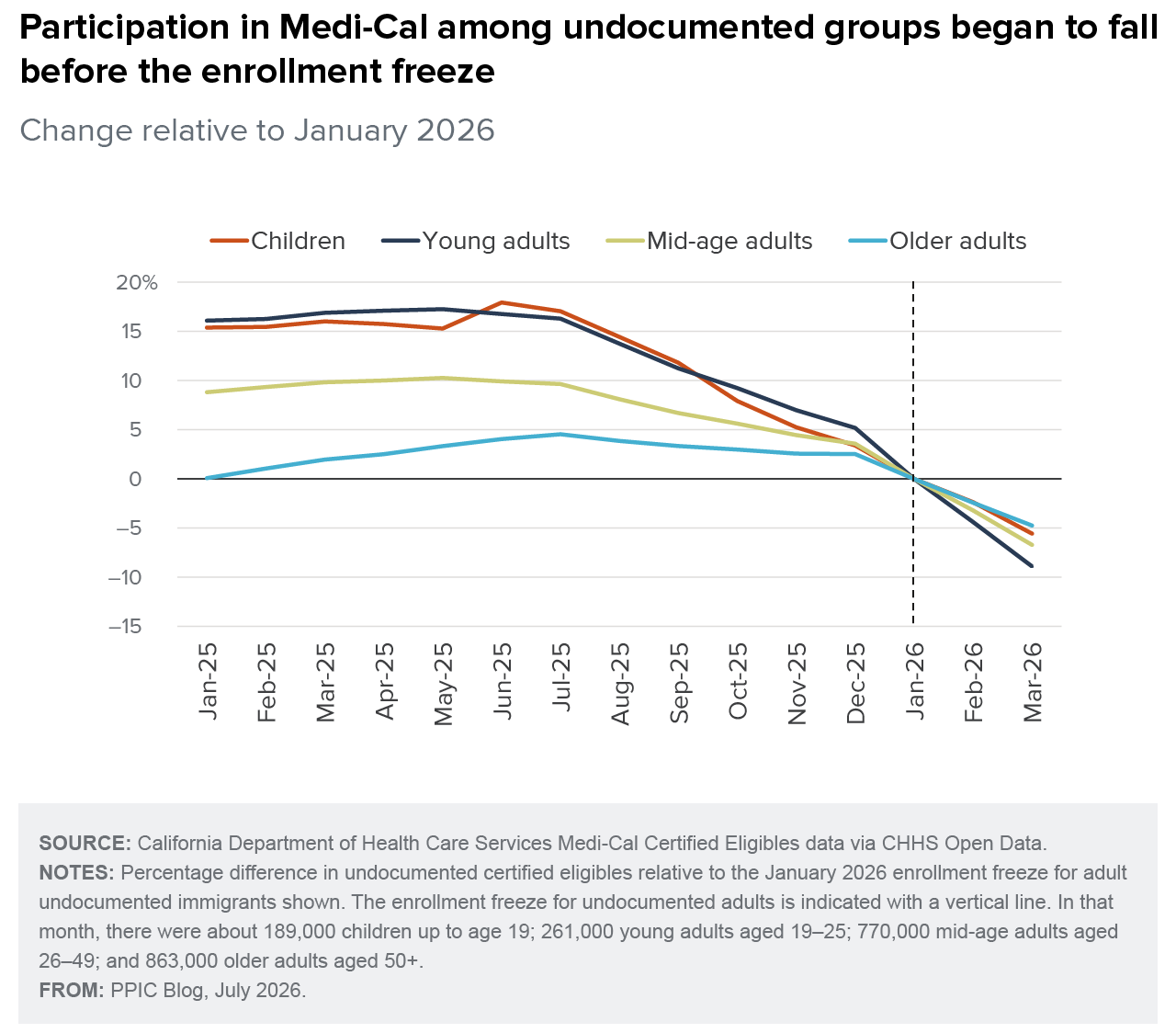
The decrease began before the freeze, however, and several things are unusual about this. First, the enrollment freeze was an incentive for eligible undocumented residents to enroll before the end of 2025, not to disenroll. Second, enrollments began to decrease much earlier in 2025, around summer, following a long upward trend. And finally, enrollment decreased for all age groups, including children, who are not affected by the freeze or most other state changes to the program.
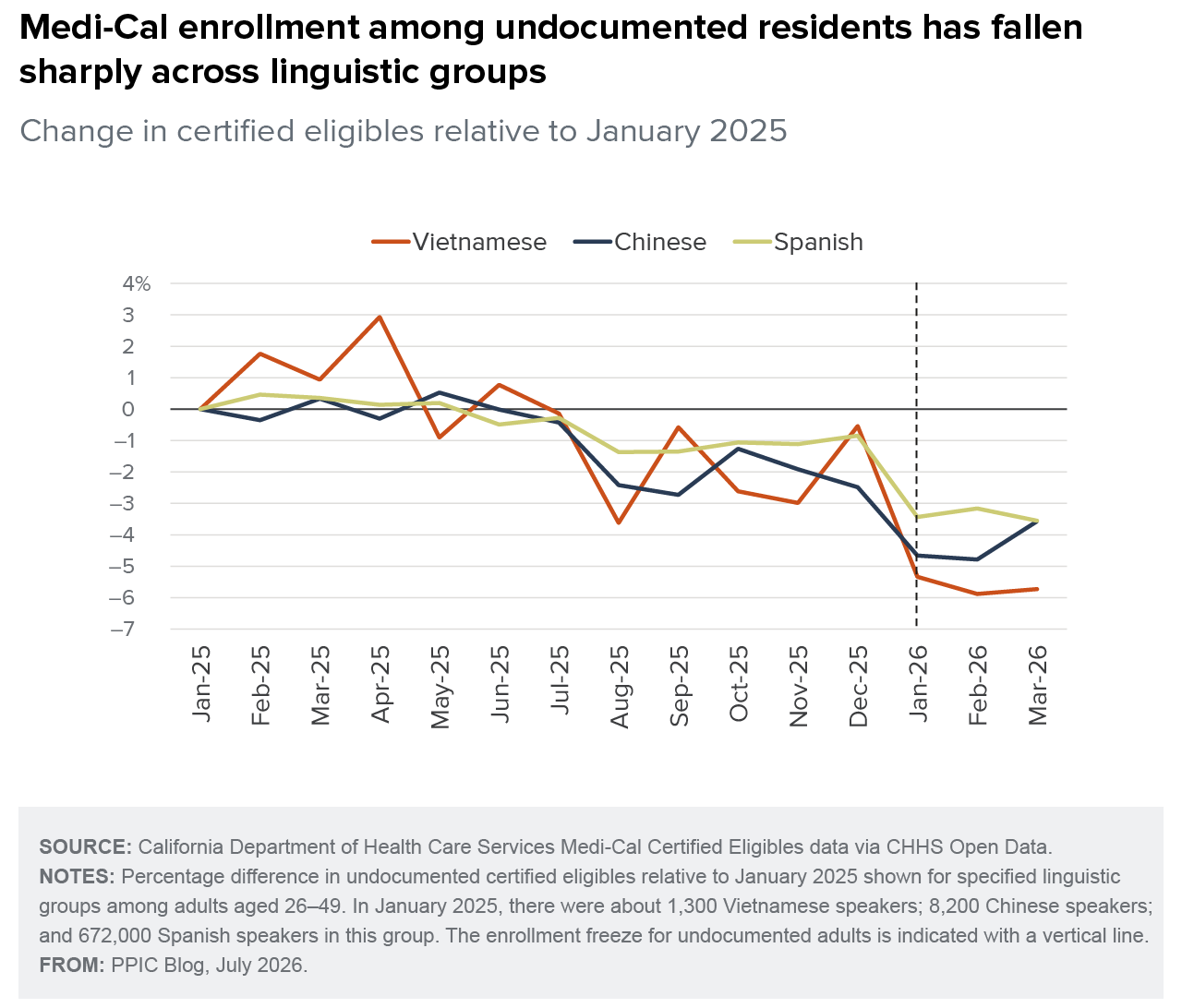
Declines beginning in mid-2025 seem to be consistent across linguistic groups, with sharp drops in enrollment among Spanish-, Chinese-, and Vietnamese-speaking adults. If these declines are disproportionately concentrated among people who believe they can do without health insurance, it could mean that the sickest enrollees remain on Medi-Cal, driving up average costs.
Federal policy changes will reduce total enrollment further, shrinking California’s General Fund obligations to Medi-Cal. However, open questions remain as to who will pay for the state’s growing uninsured population. County programs for the medically indigent used to play this role, although eligibility and benefits varied across counties.
In the current budget and federal policy environment, there are no easy solutions for meeting the health needs of all California residents. However, partial solutions can be strengthened, and improvements can be iterated over time. Safety net providers such as community health centers, county hospitals, and emergency departments will adjust to serving increasing populations in need as the state discusses strategies such as raising cost-sharing where possible, reducing covered benefits, or tapping state, county, or private sector resources to weather the budget crunch.


