Table of Contents
- Key Takeaways
- Introduction
- Health Needs Statewide and in LA County
- Health Care Visits for Undocumented versus Medi-Cal Patients
- Undocumented Older Adults and Medi-Cal Expansion
- Barriers to Care for LA’s Undocumented Immigrants
- Conclusion and Recommendations
- Notes and References
- Authors and Acknowledgments
- PPIC Board of Directors
- Copyright
Key Takeaways
California has been investing in its immigrant population by expanding Medi-Cal eligibility by age, regardless of immigration status. The final expansion to all ages will be in January 2024. To provide evidence for future health care needs, we study the health conditions and the use of health services among low-income undocumented immigrants in 350 of California’s community health centers (CHCs).
- Statewide, undocumented immigrants are about as likely as current Medi-Cal patients to have at least one chronic condition. In Los Angeles County, home to the largest immigrant population, mid-age and older undocumented patients are more likely to have at least one chronic condition.→
- Undocumented immigrants tend to receive important types of preventive services, such as the flu shot, at rates comparable to Medi-Cal patients. However, being undocumented tends to be associated with a lower likelihood that visits are coded by health care providers specifically for preventive care.→
- Older undocumented immigrants get age-appropriate health services such as cancer screenings and the shingles vaccine at rates at least as high as Medi-Cal patients. Older adults also appear to make more visits and more visits paid by Medi-Cal following expansion; we did not find these patterns among young adults.→
- Undocumented patients switched from making in-person visits to getting telehealth at similar rates to Medi-Cal patients statewide.→
- Undocumented status is associated with a higher likelihood that visits are for behavioral health. We heard about high rates of trauma among undocumented clinic patients, with a resulting high demand for counseling services.→
With the coming final expansion, county welfare departments, CHCs, and immigrant-serving organizations can expect an increased volume of Medi-Cal applicants who will need accurate information, enrollment assistance, and language services—along with access to behavioral health services. If resources allow, hiring more bi- or multilingual staff can help clinics prepare for coming increases, while expanding language and technological support for telehealth may help ease barriers to care.
Introduction
California has approximately 2 million undocumented immigrants, a group that faces considerable barriers to health care. Undocumented immigrants are less likely to have a usual source of care and are more likely to miss a doctor’s appointment due to cost, compared to other immigrants (Cha and McConville 2021a), all of which make it difficult to know whether health care needs differ for undocumented immigrants compared to other groups.
The health needs and patterns of care for this group have important implications for the state’s workforce, which is likely to rely more on immigrants as California’s native-born population ages (Johnson and Cuellar Mejia 2020). It can also inform our expectations of how quickly health care costs will grow in the state, a focus of California’s newly formed Office of Health Care Affordability. To guide the state’s investments, more nuanced information is needed about the health needs of undocumented immigrants.
Beginning in 2016, California began implementing a series of policies expanding the comprehensive version of Medi-Cal to low-income undocumented immigrants. These expansions are funded mostly with state dollars and apply to specific age groups. The largest and final age group of undocumented immigrants—26 to 49—will become eligible for Medi-Cal in January 2024. This group may have faced substantial barriers to care up to now, raising questions about their health needs and engagement with providers.
California has substantially expanded access to health care in the past decade. As part of the Affordable Care Act (ACA), it expanded Medi-Cal—the state’s version of Medicaid—to most low-income adults in 2014. California’s uninsured rate, and especially that of low-income residents, dropped dramatically following this change, making low-income undocumented immigrants the largest group of remaining uninsured (Cha and McConville 2020). Understanding the needs of undocumented immigrants can prepare the state for increased Medi-Cal enrollment, increased demand for health services, and health care needs that may not have been addressed for some time.
Our project describes undocumented immigrants’ health needs, how they access or delay care, the types of care they receive, and the barriers they face beyond lack of insurance. We use data from electronic health records from clinic visits across the state to analyze chronic health conditions, access to preventive and behavioral health services, screenings and vaccinations, and other indicators of getting needed health care. We also conduct a case study of Los Angeles (LA) County, which has the largest population of undocumented immigrants among California’s counties. Moreover, LA County operates My Health LA, a health program serving low-income undocumented immigrants who lack health insurance. We incorporate interview insights into our analyses in the LA case study.
Clinical data on visits, measurements, procedures, and diagnoses answer questions about health and health care access for a broad sample of undocumented immigrants in California. We focus on care received in community health centers (CHCs), clinics that are key health care access points for immigrants, including undocumented immigrants.
We study the health care needs of undocumented patients in terms of the prevalence of chronic diseases for this group. We examine whether undocumented patients use various types of preventive care, including cancer screenings and other services for middle-aged and older adults since older individuals may suffer negative effects from having experienced barriers to care for years. We do the same for behavioral health—which includes mental health and substance use disorder services—since this is another key component of comprehensive primary care.
While we know that not having access to insurance such as Medi-Cal is a barrier to getting health care, we investigate other important barriers that are specific to the undocumented experience. Throughout the report, we compare low-income undocumented immigrants who would qualify for Medi-Cal but for their immigration status, to Medi-Cal patients in the same clinics. Medi-Cal clinic patients make a helpful comparison group, especially since undocumented patients will join Medi-Cal in January 2024 (See Technical Appendix A for details).
Big Events and Policy Changes Occurred during the Study
Our study covers January 2018 to November 2022, a period that includes several years of the COVID-19 pandemic and two state expansions of Medi-Cal to undocumented immigrants (Figure 1). The pandemic disrupted health care substantially, with many providers and patients switching to telehealth to avoid in-person interactions. Of greater concern, the length of the pandemic led many individuals to miss important primary care visits, vaccinations, and screenings (Greiner et al. 2022; Smith and Perkins 2022; Song et al. 2021).
Large policy changes to health care occurred during the study period
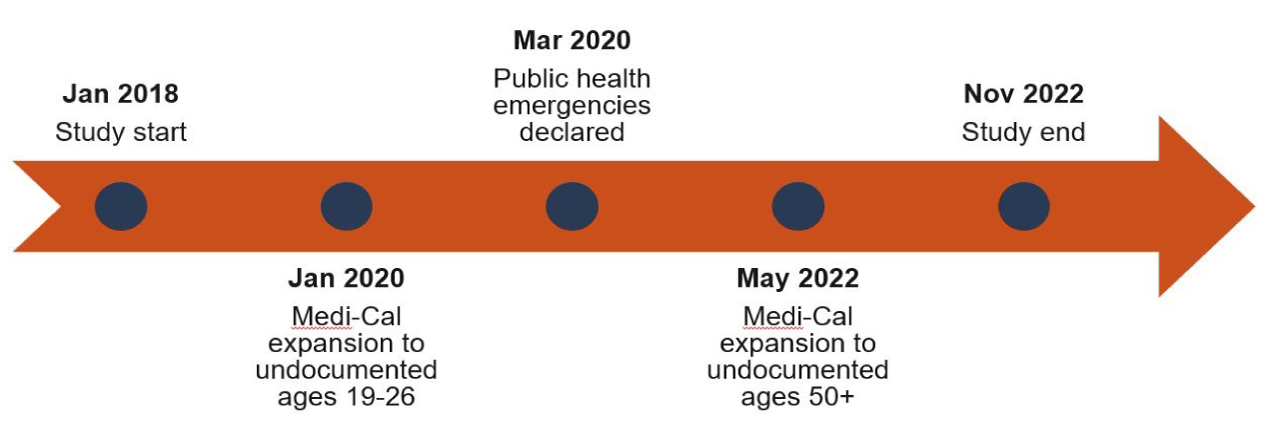
NOTE: The January 2020 expansion affects low-income adults ages 19 to 25 (26th birthday), and the May 2022 expansion affects low-income adults ages 50 and older.
Some undocumented immigrants became eligible for Medi-Cal
Since 2016, California has been expanding full-scope Medi-Cal across age groups of undocumented immigrants (Table 1). During our study period, the program expanded to low-income undocumented young adults and older adults. The final group of undocumented adults ages 26 to 50th birthday will become eligible for Medi-Cal in January 2024 if they meet income requirements; this age group makes up about 59 percent of undocumented adults in California. In this report, we refer to the policy expansion groups using the names in Table 1: children, young adults, older adults, and mid-age adults; note that “mid-age” includes a wide range of ages, including people in their 20s.
Expansions of full-scope Medi-Cal to undocumented immigrants are being rolled out by age group
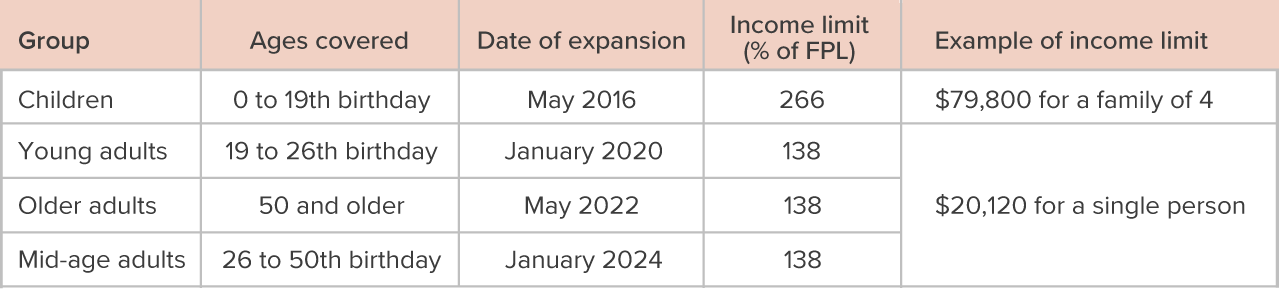
SOURCE: US Department of Health and Human Services Poverty Guidelines 2023.
NOTES: FPL is federal poverty level. The 2016 expansion to undocumented children does not affect study participants, all of whom are adults.
Telehealth went from a negligible share of visits to the majority
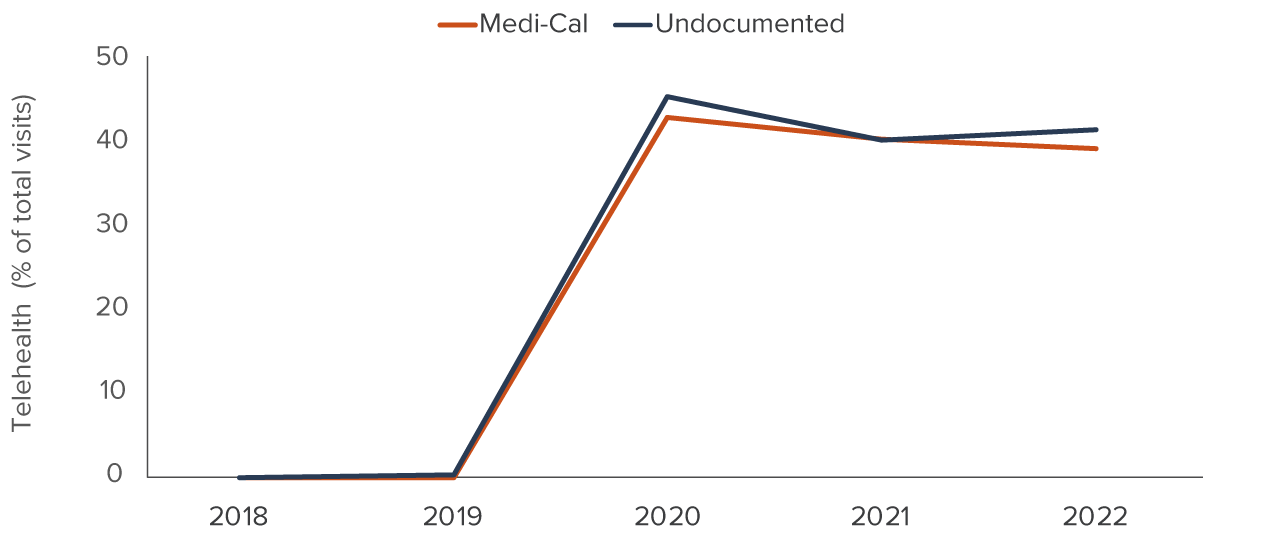
Telehealth visits made up a negligible percent of CHC visits before the pandemic (Figure 2). Federal and state declarations of a public health emergency in March 2020 relaxed many policies and requirements related to telehealth. Flexibilities included increasing telehealth reimbursements to be on par with in-person visits, and allowing providers to use previously unapproved videoconferencing software to connect with patients (US Department of Health and Human Services 2023). As a result, telehealth use in California exploded in the spring of 2020 (California Department of Health Care Services 2022; Figure 2).
Telehealth use jumped in California community health centers due to the COVID-19 pandemic
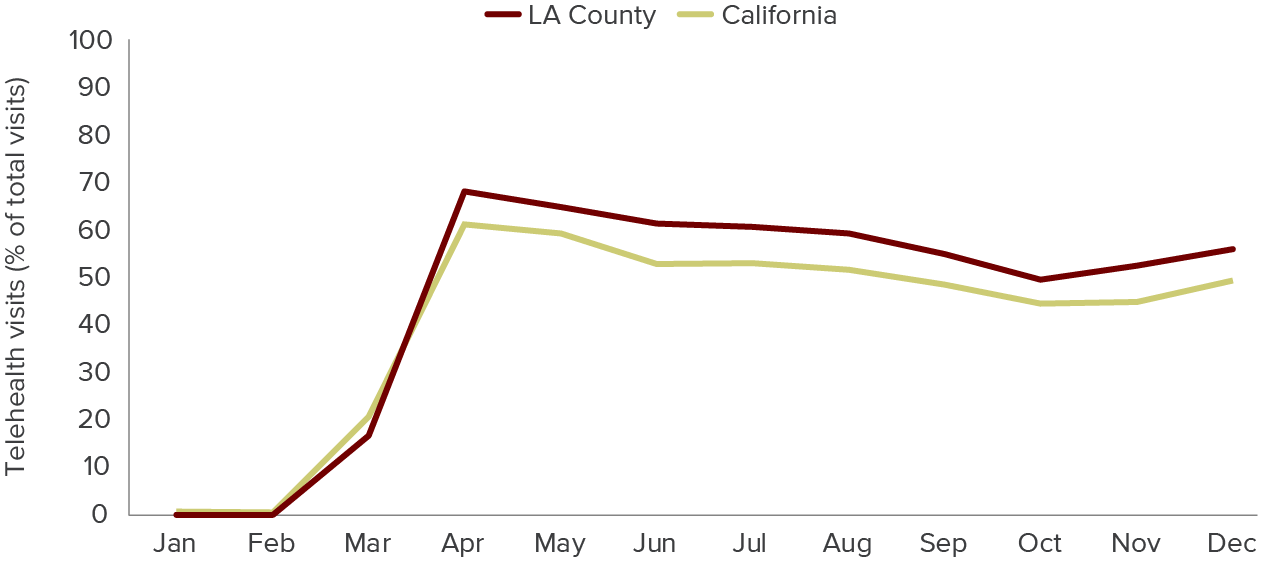
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California community health centers.
NOTES: Trends of monthly percentage of visits occurring over telehealth presented for study patients at an OCHIN member community health center in California and in Los Angeles County in 2020.
Health Needs Statewide and in LA County
Getting regular primary care, including annual wellness visits, is important for all adults. But it is especially important for individuals with chronic conditions that need ongoing management. One of the big unknowns about undocumented immigrants is whether they are healthier than other groups, and we study common chronic conditions as a way to understand their health needs.
We analyze whether study members have documentation of several common chronic conditions: asthma, diabetes, high blood pressure, high blood cholesterol, obesity, and heart disease. Though the conditions can be diagnosed during a visit or be calculated from intake measurements (as in the case of obesity), we consider only whether a health care provider has elevated the condition to a “problem list.” The problem list is part of a patient’s electronic health record that providers can access at a glance, and its use is a common practice standard.
Statewide, we study 369,891 unique individuals who made 5,460,674 CHC visits between January 2018 and November 2022. We use electronic health records from OCHIN community health centers across California that participate in the ADVANCE network (see text box).
- The undocumented and Medi-Cal comparison groups are around 42 years old on average, and 39 percent male.
- Average family size is around 2.3 to 2.5 members for both groups.
- The undocumented group is more likely to be Latino (72% vs. 47%) compared to Medi-Cal members and less likely to be white (14% vs. 25%), Black (7% vs. 12%), or Asian (6% vs. 14%).
- English or Spanish are the preferred languages. Nearly all of the statewide study members have English or Spanish as their preferred language, although the undocumented group is less likely to list English (40% vs. 67%) and more likely to list Spanish (57% vs. 23%) compared to the Medi-Cal group.
Younger Undocumented Immigrants Tend to Be Healthy but Age Brings Chronic Conditions
Statewide, undocumented immigrants have similar rates of having a chronic condition as Medi-Cal patients, with undocumented young adults being healthier than their Medi-Cal peers. Younger adults have a health advantage among the age groups in our analyses, including a lower likelihood of having any recorded chronic condition associated with being undocumented.
Chronic diseases are more common among mid-age and older adults. Over a quarter of study participants (25.9%) have one of the above conditions recorded on their problem list. However, we found no greater likelihood that being undocumented was associated with any of the chronic conditions outcomes—but undocumented status was associated with a lower likelihood of heart disease (see Technical Appendix Tables B2 and B3).
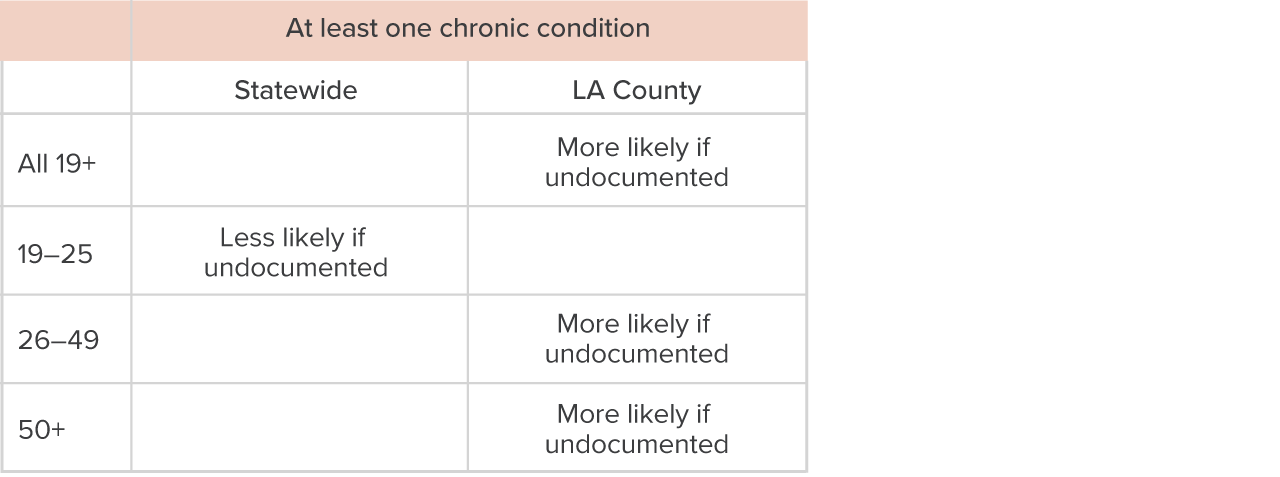
- Statewide, age and undocumented status are not associated with a patient having any recorded chronic condition, with young adults (19–25 years old) having a lower likelihood of a chronic condition.
- In Los Angeles County, age and undocumented status are associated with a patient having any recorded chronic condition, with patients in the mid-age (26–49 years old) and older (50+) groups having an increased likelihood of a chronic condition (Table 2).
How undocumented status is associated with having at least one chronic condition
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California and LA County community health centers.
NOTES: “More likely if undocumented” indicates that undocumented status is significantly associated with a greater likelihood of having at least one chronic condition, “Less likely if undocumented” indicates that undocumented status is significantly associated with a lower likelihood, and a blank box indicates no (significant) association. Chronic conditions include asthma, diabetes, high blood pressure, high cholesterol, obesity, and heart disease. The likelihoods describe regression-adjusted estimates in Technical Appendix Tables B2, B3, B5, and B6. The regressions are linear probability models of the likelihood of having at least one of these conditions associated with undocumented status. Control variables include age on first day of the study, sex, race/ethnicity, preferred language, as well as fixed effects for county (clinic in LA County). Standard errors are clustered by county (clinic). Effects are considered significant if they differ from 0 at the 95 percent level of confidence or greater.
We Highlight Los Angeles County Because It Is a Hub for Immigrant Communities
At 10 million residents as of January 2023, Los Angeles County is California’s most populous county. LA County also has the largest number of undocumented immigrants of any California county; there are approximately 614,000 undocumented adults ages 19 and older living in LA County, or roughly 32 percent of the state’s undocumented immigrants in this age range.
The city and county of LA have been especially welcoming of immigrants, creating the Office of Immigrant Affairs at the county level and the LA Mayor’s Office of Immigrant Affairs to provide services and resources for immigrant and refugee Angelenos. The county is home to large communities originally from China, El Salvador, Guatemala, Iran, Korea, Mexico, the Philippines, Vietnam, and other countries (Crable 2020).
We conduct separate analyses in Los Angeles (LA) County, where we analyze 1,077,678 CHC visits for 70,299 patients.
- Undocumented LA study members are around 46 years old, slightly older than Medi-Cal comparison group members, who are around 42.
- The LA undocumented group is slightly less likely to be male than the comparison group, 38 percent versus 44 percent.
- Undocumented LA patients have larger family sizes, with around 2.3 members, compared to 1.8 for the Medi-Cal comparison group.
- Undocumented study members in LA are more likely to be Latino (80% vs. 52%), and they are less likely to be any other race group than Medi-Cal study members (white 8% vs. 19%; Black 6% vs. 22%), although a similar proportion are Asian (5% vs. 6%).
- English and Spanish together make up 98 percent of LA study members’ preferred languages, although the proportions are uneven: 29 percent of undocumented members prefer English compared to 70 percent of Medi-Cal members. Spanish makes up almost all of the other language preferences among study members (69% for undocumented, 28% for Medi-Cal).
In discussing LA County findings, we incorporate qualitative insights from experts when they are available and relevant—primarily on the topics of behavioral health, telehealth, and barriers to care.
The LA study patients and their health conditions differ from the California-wide study patients
The differences in health status between the statewide and LA study groups suggest that the clinic study population in LA differs from the study group in the rest of California. In LA County, we find higher rates of recorded chronic disease among undocumented patients (see Technical Appendix Tables B5 and B6).
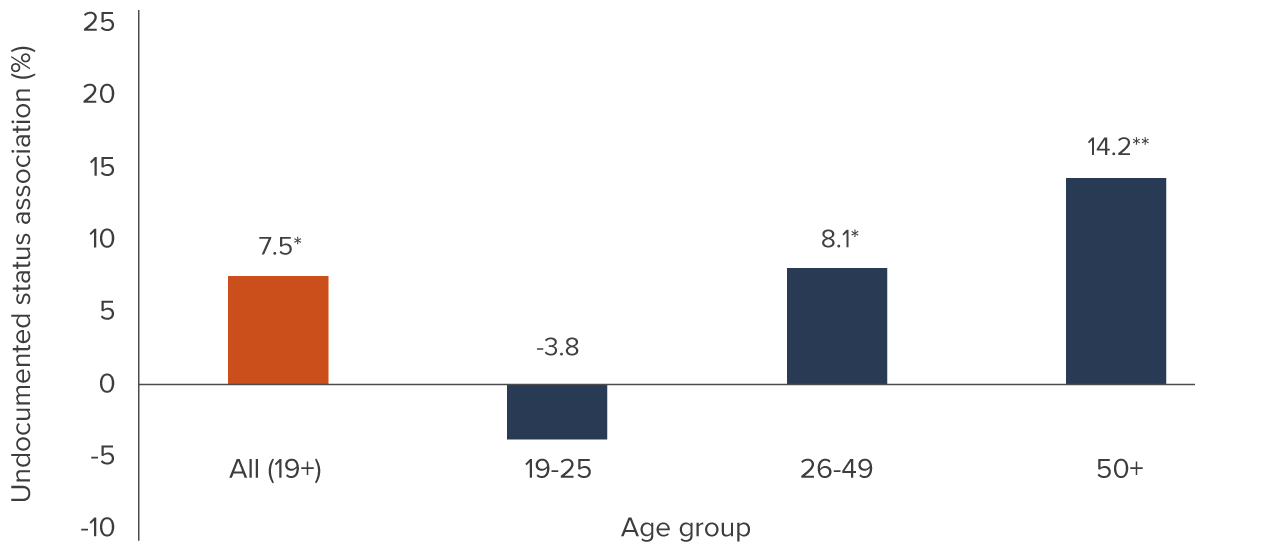
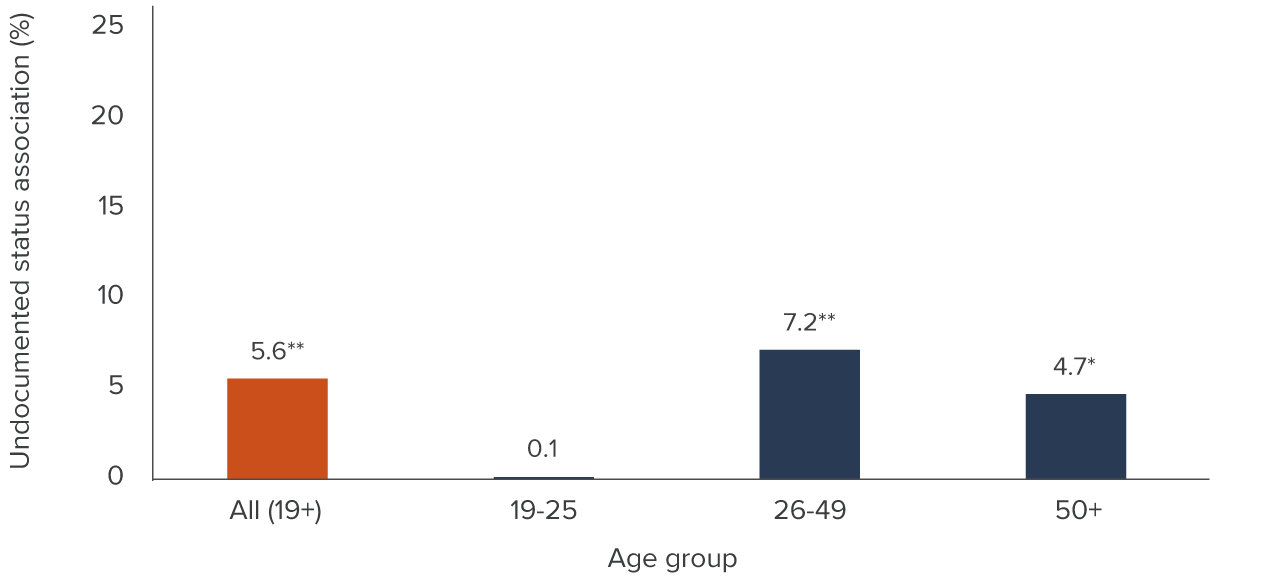
- In LA, about 34.6 percent of study patients have at least one of the chronic conditions we analyze. Being undocumented is associated with a 7.5 percent higher likelihood of having at least one chronic condition (Figure 3).
While the difference is not large, it is notable, and the fact that older ages are most affected (14.2% higher vs. no difference for young adults) suggests greater health needs in the recent and coming Medi-Cal expansion groups. There is also the possibility that some health systems in the LA County study disproportionately screen and evaluate for these conditions. Likelihood of asthma, high blood pressure, high cholesterol, and heart disease were similar across the undocumented and Medi-Cal groups; average rates of these conditions ranged from 0.9 percent for heart disease to 18.8 percent for high cholesterol.
In LA County, the higher likelihood of any recorded chronic disease among undocumented adults is driven by diabetes and obesity.
- About 10.6 percent of study members in Los Angeles have diabetes, and being undocumented is associated with a 2.1 percentage point (19.8%) increase in the likelihood of having diabetes.
- About 16.2 percent of LA study members have obesity, and being undocumented is associated with a 1.7 percentage point (10.5%) increase in the likelihood of having obesity.
Undocumented patients in LA County are more likely than Medi-Cal patients to have at least one chronic condition
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s LA County community health centers.
NOTES: Bars represent regression-adjusted associations between having a recorded chronic disease and undocumented status, scaled by mean outcome. Regressions are linear probability models of the likelihood of having any chronic disease associated with undocumented status. See Technical Appendix Tables B5 and B6 for model estimates. Chronic diseases include asthma, diabetes, high blood pressure, high cholesterol, obesity, and heart disease. Control variables include age on first day of the study, sex, race/ethnicity, preferred language, as well as fixed effects for clinic in LA County. Standard errors are clustered by clinic. Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
*p<0.05 **p< 0.01
One notable difference is that LA is overwhelmingly urban and suburban, whereas the state overall has greater diversity of urbanicity. Agricultural parts of the state employ many undocumented immigrants, and agricultural workers are more likely to be healthy, given the strenuous nature of their jobs (Zavodny 2015). Another possible difference is that certain LA clinics could be especially focused on conducting some types of screening and evaluation.
Health Care Visits for Undocumented versus Medi-Cal Patients
Preventive and behavioral health are key outcomes because they are fundamental components of health care that low-income uninsured individuals may forgo due to cost or other access barriers. We analyze whether visits to clinics by patients in our study fit into four broad categories: those including preventive health care such as annual checkups; behavioral health, which encompasses both mental health and substance use disorder services; and telehealth-delivered visits of any type. Technical Appendix A explains how we used information about providers and visits to define these categories. We also analyze associations with undocumented status among all adults as well as within age groups, statewide and in LA County.
Visits by Undocumented Immigrants Are Less Likely to Be Specifically for Preventive Care
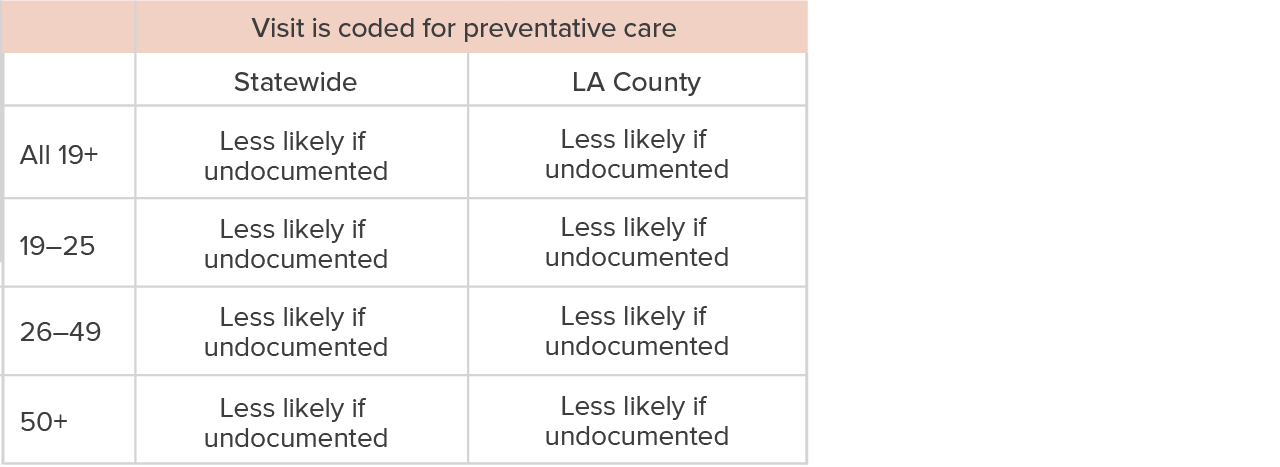
Most clinic visits by study members statewide (55.9%) and in LA County (66.8%) are coded for preventive health services, reflecting the mission among community health centers to deliver primary care to underserved populations. Visits can include preventive care even if they are not coded as preventive care visits, so these numbers likely underestimate the amount of preventive care our study members receive. Undocumented patients statewide and in LA County are less likely to visit a CHC only for preventive care, compared to Medi-Cal patients (Table 3).
- Statewide, visits by undocumented patients are 20 percent less likely to be coded as preventive care (see Technical Appendix Tables B9 and B10).
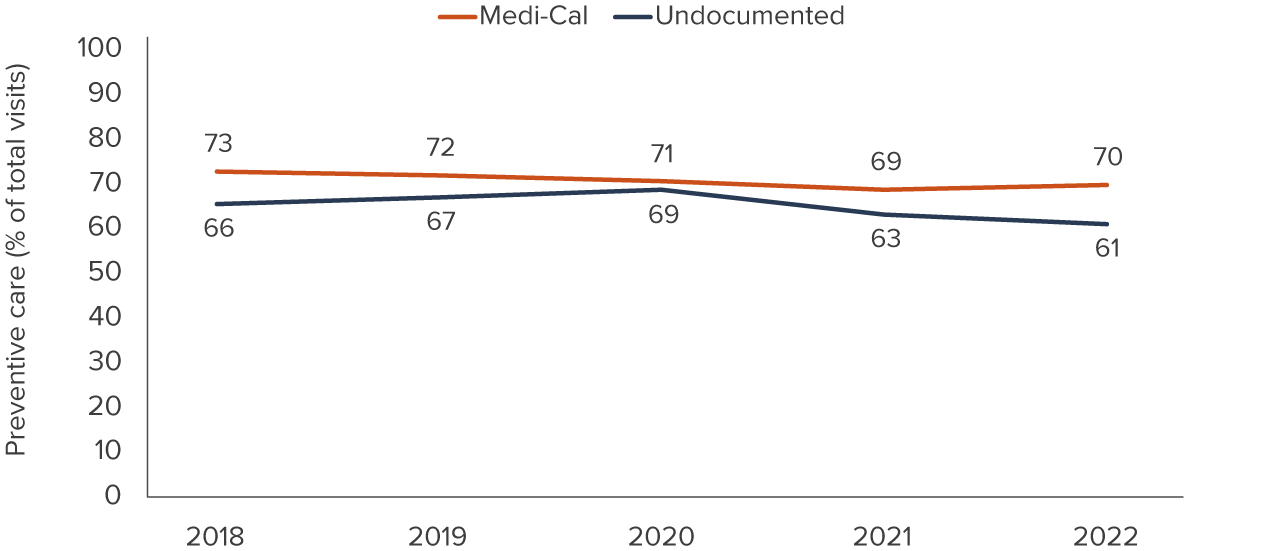
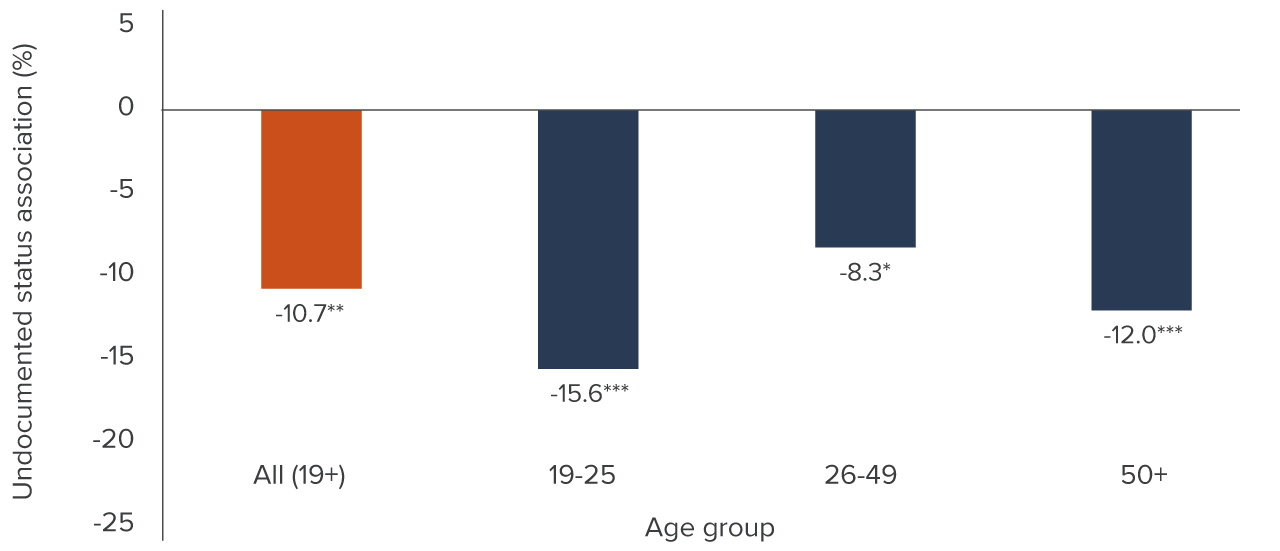
- In LA County, the percentage of preventive care visits is lower over the study period and persists despite year-to-year fluctuations (Figure 4). We estimate nearly an 11-percent lower likelihood of visits coded as preventive care relative to the county average (see Technical Appendix Tables B11 and B12); as in the statewide findings, this is true across age groups (Figure 5).
How undocumented status is associated with preventive care visits
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California and LA County community health centers.
NOTES: “Less likely if undocumented” indicates that undocumented status is significantly associated with a lower likelihood of a visit being coded for preventive care by the health care provider, where these characteristics describe regression-adjusted estimates of the coefficient on undocumented status. Regressions are linear probability models of the likelihood of visit type associated with undocumented status. See Technical Appendix Tables B9, B10, B11, and B12 for model estimates. Control variables include age at visit, sex, race/ethnicity, preferred language, as well as fixed effects for county (clinic in LA County) and calendar year. Standard errors are clustered by county (clinic). Effects are considered significant if they differ from 0 at the 95 percent level of confidence or greater.
A lower share of undocumented patients’ visits are coded for preventive health care compared to Medi-Cal patients in Los Angeles County
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s LA County community health centers.
NOTES: Trends of annual percentage of visits for preventive health services presented for undocumented and Medi-Cal patients at an OCHIN member community health center in Los Angeles County.
Undocumented patients are less likely to have visits coded as preventive care in LA County
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s LA County community health centers.
NOTES: Bars represent regression-adjusted associations between a visit being coded for preventive care and patient undocumented status, scaled by mean outcome. Regressions are linear probability models of the likelihood of having a preventive care coded visit associated with undocumented status. See Technical Appendix Tables B11 and B12 for model estimates. Control variables include age on the day of the visit, sex, race/ethnicity, preferred language, as well as fixed effects for clinic and calendar year. Standard errors are clustered by clinic. Effects are considered significant if they differ from 0 at the 95 percent level of confidence or greater.
*p<0.05 **p< 0.01 ***p<0.001
We cannot distinguish whether undocumented patients receive less preventive care in total, or if they receive preventive care during visits for specific concerns. In terms of how meaningful the differences between groups are, the average study member statewide makes about 15 clinic visits, about 8 of which are coded as preventive care visits. The 20 percent lower likelihood among undocumented patients statewide translates to about 1.5 fewer visits on average. The difference may not seem like much, especially with the limitations of our interpretation, but our estimates are significant and consistent across age groups, which indicates that a clear difference is likely in the patterns of how undocumented immigrants seek or receive care.
Undocumented Patients Get Cancer Screenings at Rates at Least as High as Their Medi-Cal Peers
Preventive care is a broad concept, and we are especially interested in whether undocumented immigrants receive certain health services that start to be recommended around middle age. The largest group of undocumented immigrants ineligible for Medi-Cal, those ages 26 to 49, and the most recently eligible group, ages 50 and older, include adults who should receive certain age-appropriate health services.
Breast and colon cancer are types of cancer for which early detection can improve outcomes and reduce the risk of death (National Cancer Institute 2021). Screening is an option for both. We analyze the relationship between undocumented status and receiving recommended health services for breast cancer screenings for women over 50, and colon cancer screenings for adults over 45.
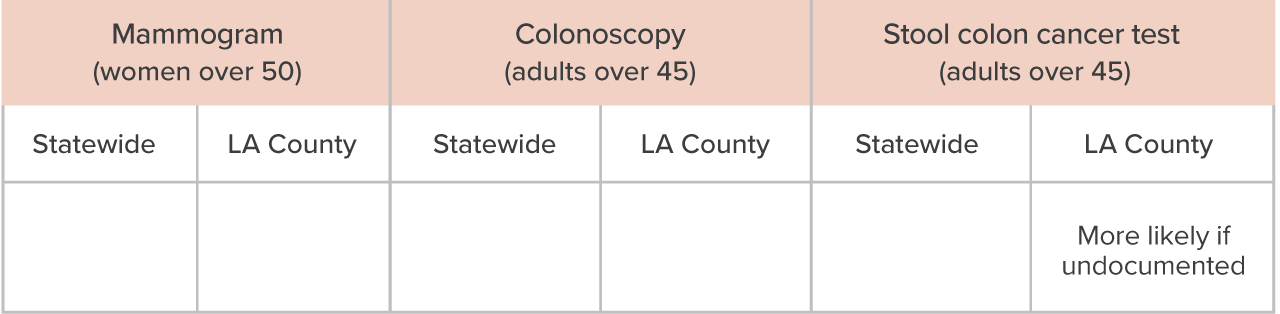
- Statewide, there was no association between being undocumented and getting a mammogram, a colonoscopy, or a stool colon cancer test.
- In LA County, there was no association with mammograms or colonoscopies and undocumented status, but undocumented patients did have a higher likelihood of conducting a stool colon cancer test.
Table 4 summarizes our findings for the screenings recommended for mid-age and older adults. We discuss these findings, followed by related findings on cervical cancer screening for adult women.
How undocumented status is associated with receiving breast and colon cancer screenings
SOURCE: ADVANCE network data for low-income patients in indicate age/sex groups who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California and LA County community health centers.
NOTES: “More likely if undocumented” indicates that undocumented status is significantly associated with a greater likelihood of receiving the described screening, and a blank box indicates no (significant) association. These characteristics describe regression-adjusted estimates in Technical Appendix Tables B13 and B14. Control variables include age on first day of the study, sex, race/ethnicity, preferred language, as well as fixed effects for county (clinic in LA County). The regressions are linear probability models of the likelihood of receiving screenings associated with undocumented status. Standard errors are clustered by county (clinic). Effects are considered significant if they differ from 0 at the 95 percent level of confidence or greater.
Mammograms and colonoscopies are completed by undocumented, Medi-Cal patients at similar rates
Guidance for when women should have a mammogram is in flux and varies across professional medical societies (Bever 2023), but during the study, screening was typically recommended for women 50 and older.
- Statewide, about 33.9 percent of women aged 50 or older at the beginning of the study had a completed mammogram on file by the end of the study.
- In LA County, 23.1 percent had a completed mammogram on file.
All study members had a minimum of around two years of follow up, making these rates quite low compared with the national rate of 76 percent of women ages 50 to 74 getting screened in the past two years (National Cancer Institute 2021).
- Though study members’ rates are low, being undocumented is not associated with any significant difference in the likelihood of getting a mammogram (see Technical Appendix Tables B13 and B14).
Colonoscopy and the fecal occult blood test are two procedures used to screen for colon cancer. For years, guidelines recommended that adults receive their first colonoscopy at age 50, but updated guidelines recommend beginning at 45 due to increasing prevalence of colon cancer at younger ages (de Kanter, Dhaliwal, and Hawks 2022). Since our study spans the change in guidelines, we include adults aged 45 and older at the start of the study and analyze whether they have a colonoscopy on file by the end of the study. The fecal occult blood test checks stool for hidden blood, a potential indicator of cancer.
- Statewide, about 3.7 percent of the study group receive a colonoscopy.
- In LA County, 1.9 percent receive a colonoscopy during the study.
- Statewide, 42.5 percent of the study group completed the fecal occult blood test.
- In LA County, 53.4 percent completed the fecal occult blood test.
Colonoscopies are recommended every 10 years and the stool test is recommended annually. As a rough calculation, if patients are getting screened as recommended, we would expect their ever-screening rates to be over 10 percent for colonoscopy and over 100 percent for the stool test (expected rates in the first study year alone). Nationally, about 72 percent of adults ages 50 to 75 receive colon cancer screenings as recommended (National Cancer Institute 2021), much higher than our study participants. Calculating our rates beginning at age 50 does not change our conclusions.
- Being undocumented is not associated with any significant difference in likelihood of having a colonoscopy, statewide or in LA. (See Technical Appendix Tables B13 and B14.)
Analyses of colonoscopy are similar to those for mammography. Findings for the stool test diverge from this pattern, however (Technical Appendix Tables B13 and B14).
- Statewide, rates for the stool test are similar between undocumented and Medi-Cal patients in the adjusted analyses.
- In LA County, undocumented status is associated with a 21 percent higher rate of completing the stool test. Notably, the stool test can be completed in the CHC and does not require a referral. Alternately, some health systems in LA County may be more likely to suggest or offer screening.
While we do not know the underlying mechanisms for these findings, the need to complete a screening through a referral out of the clinic may pose a steeper barrier for undocumented patients. Clinic-based services also may be closer or more familiar to patients than referrals.
PAP tests, like stool tests, are more likely among undocumented patients in LA County
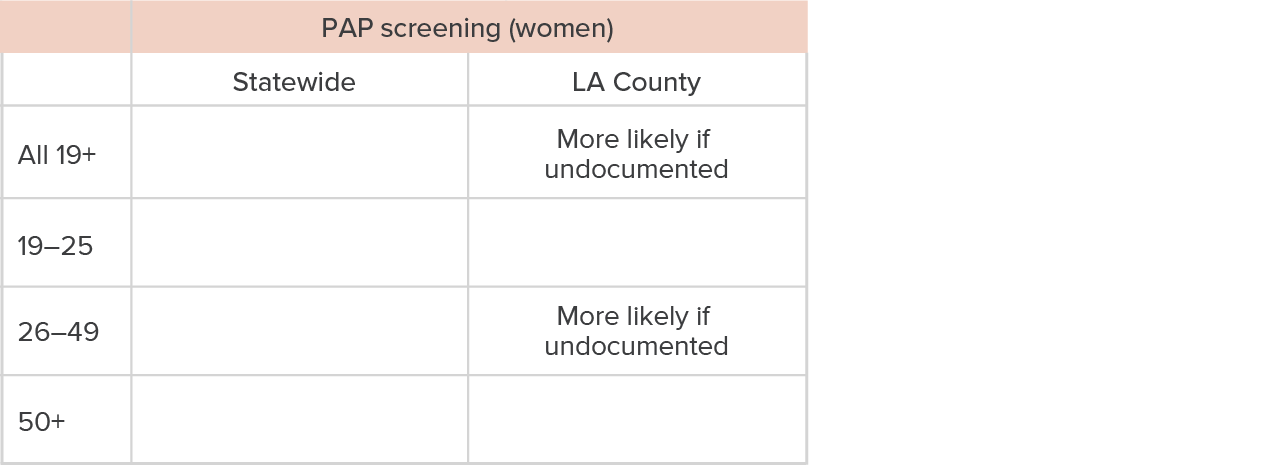
PAP tests to screen for cervical cancer are recommended for a wider range of ages than the other cancer screenings we investigate. We analyze the relationship between undocumented status and ever having a PAP test for women of all ages as well as by age group (Table 5).
- Statewide, about 37.6 percent of undocumented women in our study had a PAP test during the study.
- In LA County, about 25.8 percent of undocumented women had a PAP test.
Recommendations for test frequency can be up to every five years, which would imply an ever-screened rate of over 40 percent (we follow each patient for at least ~2 years) if patients are up to date. While some share of study women may not have received a PAP on the recommended schedule, screening for cervical cancer is closer to recommendations than breast or colon cancer screening. Nationally, about 72 percent of women ages 21 to 65 are up-to-date on PAP testing (National Cancer Institute 2021).
- Statewide, undocumented status does not change the likelihood of getting a PAP test (see Technical Appendix Tables B15 and B16). This was true for women overall, and it remained so among young, mid-age, and older women.
- In Los Angeles, however, being undocumented was associated with a 16 percent higher likelihood of being screened (Technical Appendix Tables B17 and B18), and these findings were concentrated among women ages 26 to 49. (Note: we did not adjust findings for pregnancy status, which could drive different screening rates.)
How undocumented status is associated with receiving PAP screenings
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California and LA County community health centers.
NOTES: “More likely if undocumented” indicates that undocumented status is significantly associated with a greater likelihood of receiving a PAP screening, and a blank box indicates no (significant) association. These characteristics describe regression-adjusted estimates in Technical Appendix Tables B15, B16, B17, and B18. The regressions are linear probability models of the likelihood of receiving several types of health services associated with undocumented status. Control variables include age on first day of study, sex, race/ethnicity, preferred language, as well as fixed effects for county (clinic in LA County). Standard errors are clustered by county (clinic). Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
Statewide Vaccine Take-Up Is Similar, but LA’s Undocumented Immigrants Exceed Their Medi-Cal Peers
Another key component of preventive care is getting regular vaccinations, something that became salient during the COVID-19 pandemic. We analyzed the relationship between undocumented status and patients’ likelihood of getting the shingles vaccine among adults over 50 (Table 6). We discuss this finding as well as our analyses on flu and COVID-19 vaccinations for all ages, with additional findings by age group.
Shingles vaccination is more likely among older undocumented patients in LA County
While people of all ages can develop shingles, older adults are at higher risk of developing the condition, and they are at higher risk of complications if they do develop it (Centers for Disease Control and Prevention 2019). We analyze whether study members over 50 had at least one shingles shot.
The full protocol for the currently approved Shingrix vaccine is two shots, but the previously available Zostavax was a one-shot option (Centers for Disease Control and Prevention 2023). Both were available and approved for use in adults 50 and older during our study, though Zostavax was discontinued in late 2020.
How undocumented status is associated with receiving the shingles vaccine

SOURCE: ADVANCE network data for low-income patients in indicate age/sex groups who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California and LA County community health centers.
NOTES: “More likely if undocumented” indicates that undocumented status is significantly associated with a greater likelihood of receiving a shingles vaccine, and a blank box indicates no (significant) association. These characteristics describe regression-adjusted estimates in Technical Appendix Tables B13 and B14. Regressions are linear probability models of the likelihood of receiving the shingles vaccine associated with undocumented status. Control variables include age on first day of study, sex, race/ethnicity, preferred language, as well as fixed effects for county (clinic in LA County). Standard errors are clustered by county (clinic). Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
Statewide, about 27.7 percent of older adults received a shingles shot, and in Los Angeles County, about 29 percent of older adults received a shingles shot.
- Statewide, there was no difference in likelihood of getting the shingles shot associated with undocumented status (see Technical Appendix Table B13).
- In LA County, being undocumented increases the likelihood of getting vaccinated by 23 percent, quite a large effect (Technical Appendix Table B14). This finding is similar to the other vaccine findings for Los Angeles that we describe later in this section, and fits with past work on immigrants’ vaccination rates (Heintzman et al. 2022).
In LA, in-clinic screenings and shots for older ages are positively associated with undocumented status
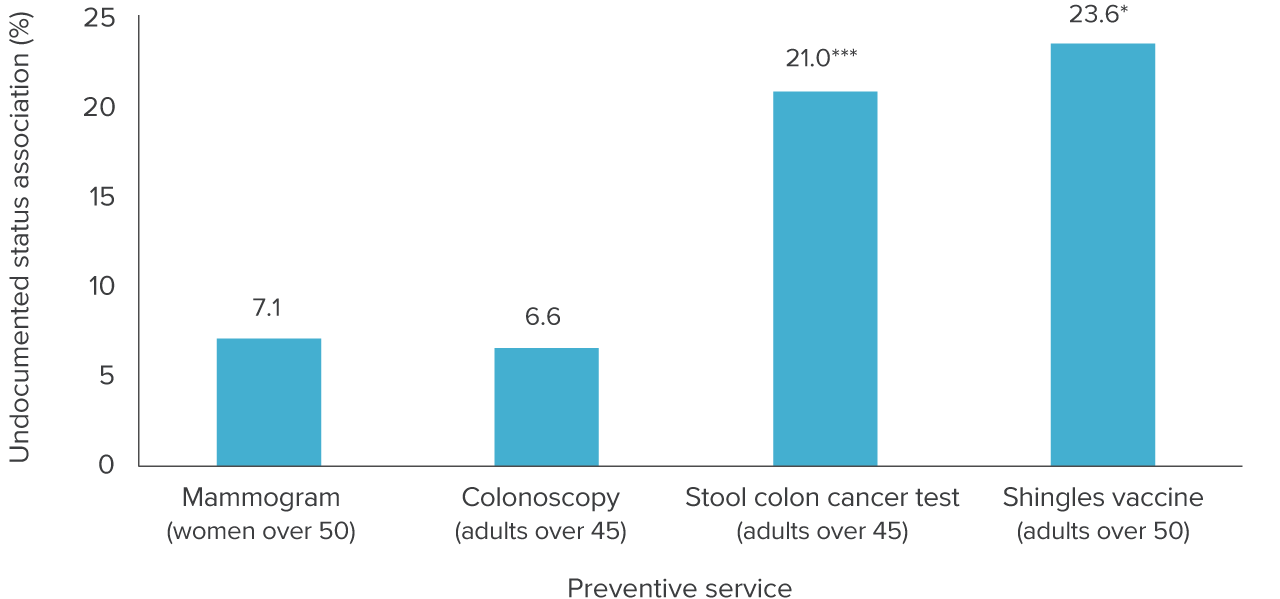
Statewide, undocumented patients get age-appropriate breast cancer screening, colon cancer screening, and shingles shots at rates indistinguishable from Medi-Cal patients. However, we found an interesting pattern (Figure 6): between groups, there was no difference in the likelihood of getting services that are referred out of the clinic, while patients with undocumented status had a high likelihood of getting a service that can be completed at the CHC. Undocumented patients may face more barriers to following up on a referral, but they are otherwise more likely to get recommended screenings. We return to the question of barriers to care for this group in a later section.
Undocumented patients are at least as likely to have certain preventive services for middle-aged adults in LA County
SOURCE: ADVANCE network data for low-income patients who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s LA County community health centers. See figure labels for age groups for each screening or shot.
NOTES: Bars represent regression-adjusted associations between having the listed screening or vaccine and undocumented status, scaled by mean outcome. Regressions are linear probability models of the likelihood of having a preventive care coded visit associated with undocumented status. See Technical Appendix Tables B13 and B14 for model estimates. Control variables include age on the day of the visit, sex, race/ethnicity, preferred language, as well as fixed effects for clinic and calendar year. Standard errors are clustered by clinic. Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
*p<0.05 ***p<0.001.
Findings for flu and COVID-19 vaccination echoed our shingles shot findings
Flu and COVID-19 vaccination are recommended for adults of all ages, and both were available through CHCs. As with other outcomes, we investigate by age group whether patients ever received these shots at a study clinic (Table 7). About 44.6 percent of adults statewide and 43.3 percent of adults in LA received at least one flu vaccine at a CHC during the study. We may be missing information on flu shots administered in other settings, such as jobs or retail pharmacies, so this is likely to be an underestimate of the percent of patients who were ever vaccinated against the flu.
- We found no significant association with undocumented status statewide, though the age group analysis revealed a negative association among young adults, who were less likely to get a flu shot if undocumented.
- In LA County, being undocumented is associated with a 19.1 percent higher likelihood of receiving a flu shot among all adults, and this positive association held for all age groups. It is, however, unclear whether the difference in LA reflects a higher propensity to get vaccinated for the flu among undocumented immigrants, or a higher propensity to get the shot at the CHC versus another place.
How undocumented status is associated with receiving flu and COVID-19 vaccines
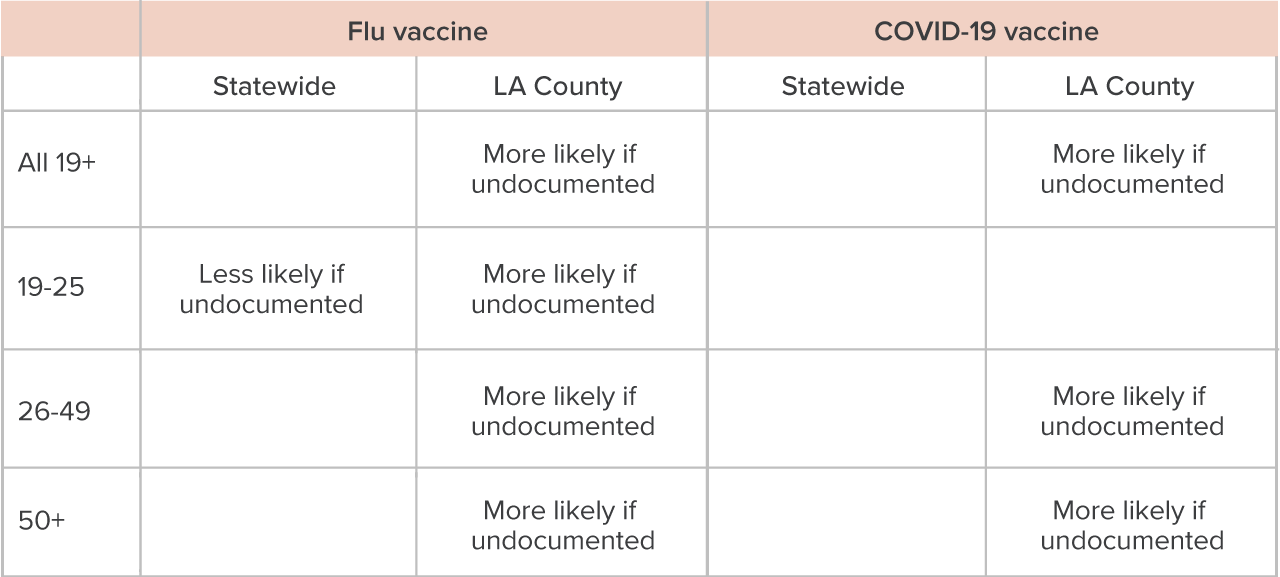
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California and LA County community health centers.
NOTES: “More likely if undocumented” indicates that undocumented status is significantly associated with a greater likelihood of receiving the listed vaccine, and a blank box indicates no (significant) association. These characteristics describe regression-adjusted estimates in Technical Appendix Tables B15, B16, B17, and B18. Regressions are linear probability models of the likelihood of receiving flu and COVID-19 vaccines associated with undocumented status. Control variables include age on the first day of the study, sex, race/ethnicity, preferred language, as well as fixed effects for county (clinic in LA County). Standard errors are clustered by county (clinic). Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
The first vaccines against COVID-19 received emergency use approval in the US in December 2020 (US Food and Drug Administration 2021), and the primary vaccine shots rolled out through the spring and summer of 2021. CHCs were among the providers on the front lines giving vaccines in underserved communities. Statewide, 55 percent of adults received at least one COVID-19 shot, and in LA County, 49 percent of adults did so. The patterns we find in the adjusted analyses have similarities to our flu shot findings. (See Technical Appendix Tables B15, B16, B17, and B18 for findings on COVID-19 and flu vaccines.)
- Statewide, there is no association with undocumented status and the likelihood of getting a COVID vaccination in at any age.
- In LA County, undocumented status is associated with a 17.2 percent increased likelihood of receiving a shot for COVID.
Providers giving these vaccines were required to report shots on a state database within 24 hours of administering them (California Department of Public Health 2022). These data were shared across providers, increasing the likelihood that COVID-19 shots administered in other locations also appear in the immunization files of study adults in CHCs—and thus represent truly higher take-up of COVID-19 vaccinations among undocumented immigrants. The effects were concentrated in the middle- and older-adult age groups in LA.
In summary, undocumented status in LA was associated with higher take-up with all of the vaccines we studied—shingles, flu, and COVID-19—as shown in Figure 7. These findings are consistent with the analyses for older adults, where we found undocumented status in LA to be associated with higher rates of in-clinic preventive services.
Undocumented patients are more likely to get vaccines in LA County clinics compared to Medi-Cal patients
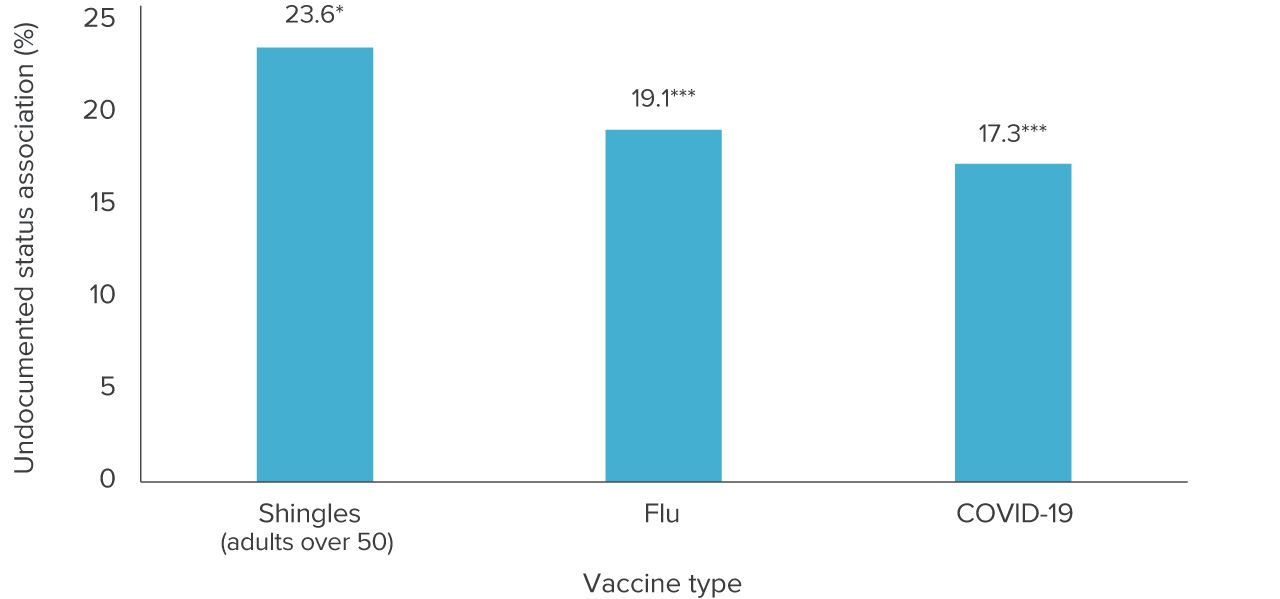
SOURCE: ADVANCE network data for low-income patients ages 19 and older (or 50 and older for shingles) who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s LA County community health centers.
NOTES: Bars represent regression-adjusted associations between having the listed vaccine and undocumented status, scaled by mean outcome. Regressions are linear probability models of the likelihood of having a preventive care coded visit associated with undocumented status. See Technical Appendix Tables B14 and B17 for model estimates. Control variables include age on the day of the visit, sex, race/ethnicity, preferred language, as well as fixed effects for clinic and calendar year. Standard errors are clustered by clinic. Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
*p<0.05 **p<0.01 ***p<0.001
Undocumented Immigrants Need, and Use, More Behavioral Health Services
Behavioral health visits, which include visits for mental health or substance use disorder, make up 10.5 percent of CHC visits statewide, and 6.6 percent in LA County.
The proportion of total visits is small, but we learned from our LA interviews that behavioral health is a growing priority for clinics, and that demand for services among patients is high. Table 8 summarizes our statewide and LA County findings by age on the association of undocumented status with behavioral health visits.
- Undocumented status is associated with a much higher likelihood that a patient’s visit is for behavioral health services statewide (36%), according to our adjusted analyses (see Technical Appendix Tables B9 through B12); the link with undocumented status was concentrated in mid-age (26-49) and older undocumented immigrants statewide.
- In LA County, undocumented status is associated with an even larger likelihood that a visit is for behavioral health (46%). The link with undocumented status was present with all ages but was notably high (over 70% higher likelihood) among young adults in LA (see Figure 8).
How undocumented status is associated with behavioral health visits
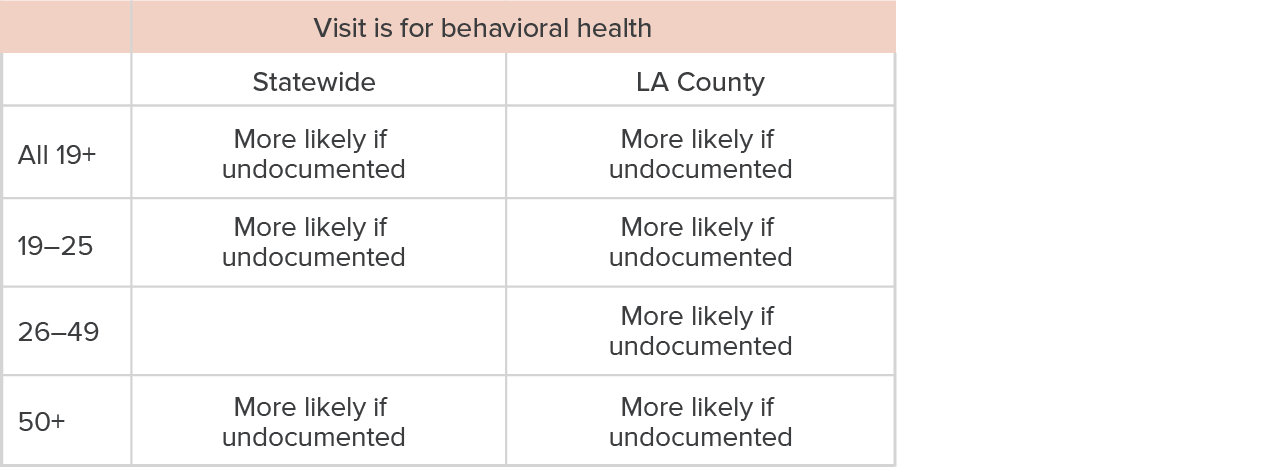
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California and LA County community health centers.
NOTES: “More likely if undocumented” indicates that undocumented status is significantly associated with a greater likelihood of visits being for behavioral health, and a blank box indicates no (significant) association. These characteristics describe regression-adjusted estimates in Technical Appendix Tables B9, B10, B11, and B12. The regressions are linear probability models of the likelihood of visit type associated with undocumented status. Control variables include age at visit, sex, race/ethnicity, preferred language, as well as fixed effects for county (clinic in LA County) and calendar year. Standard errors are clustered by county (clinic). Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
These findings were somewhat surprising, given that undocumented Latinos—who make up a large majority of the undocumented group in the study—engage less with behavioral health, according to past research in California (e.g., Ortega et al. 2018). However, several experts in our interviews shared insights supporting the findings: they report that undocumented immigrants need and use more behavioral health services because they have more trauma compared to the Medi-Cal comparison group. We heard examples of trauma related to domestic violence, the migration experience itself, and war in home countries, experiences that our interviewees said are more common among undocumented immigrants.
Visits by undocumented patients are more likely to be for behavioral health in LA County
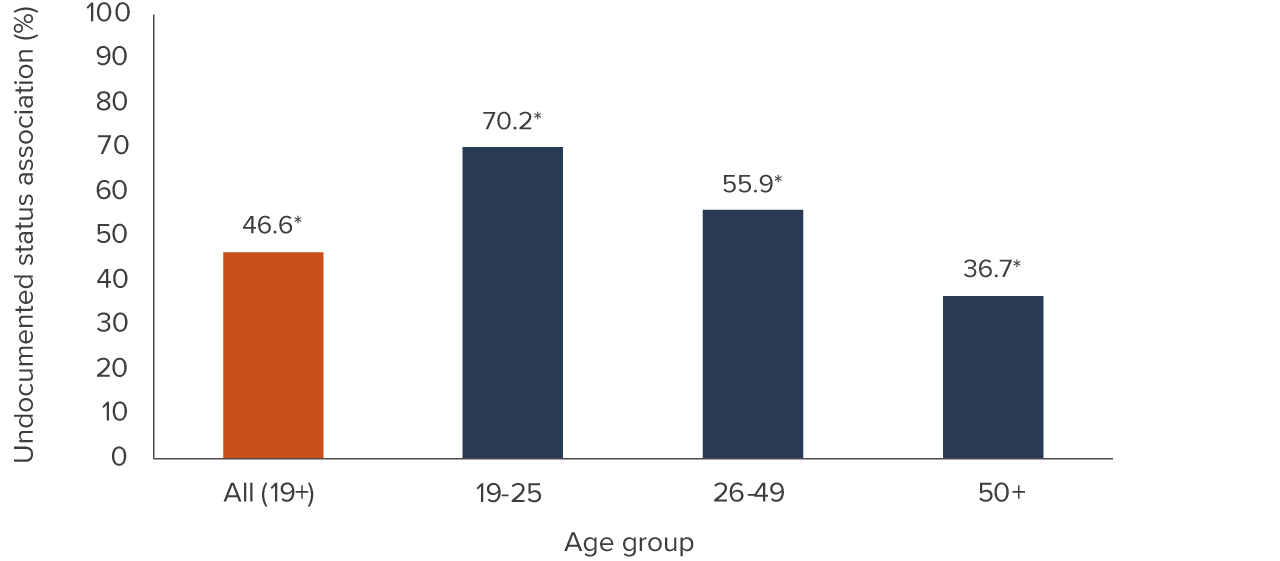
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s LA County community health centers.
NOTES: Bars represent regression-adjusted associations between visits being for behavioral health and patient undocumented status, scaled by mean outcome. Regressions are linear probability models of the likelihood of having a preventive care coded visit associated with undocumented status. See Technical Appendix Tables B11 and B12 for model estimates. Control variables include age on the day of the visit, sex, race/ethnicity, preferred language, as well as fixed effects for clinic and calendar year. Standard errors are clustered by clinic. Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
*p<0.05
We heard that many undocumented immigrant groups experience trauma, including migration-induced trauma among Mexican and Central American immigrants, Afghan refugees, domestic violence survivors, and immigrants who experience war in their home countries, according to our interviewees.
A quote from one interviewee illustrates what past trauma can look like: “A good example would be the Fourth of July. If [a patient] went through a war-torn country, and they’re hearing [fireworks]. They might not understand why they have a headache. It might be the smell, too, because fireworks emit a smell, and it might remind them of past experiences with war and how gunshots smelled in their home country.”
Trauma can lead to behavioral health and physical health issues. In one interview, we learned about how patients show symptoms with no underlying physical health issues, stemming from past trauma. After undocumented immigrants become more settled in the US, obtain stable housing and food security, and leave “survival mode,” their bodies begin to process trauma and heal. The interviewee emphasized the importance for clinical staff to engage in psychoeducation—that is, to educate patients about these connections and encourage them to seek behavioral health services and improve their health.
We also heard about trauma resulting from immigrants and their families living through poverty and being afraid of using public programs (discussed in a later section). One expert described the process: “[Patients] don’t want to renew [CalFresh] benefits after [the] first redetermination as a result of public charge fears, even when they have a need. It’s a whole vicious cycle because when the family is not very well off and they refuse to get this kind of social help, they put that burden on themselves, and when they cannot get a job to feed the family. This [cycle deteriorates] mental health, then they put their anger on their children, then the children are not doing so well because they did not get help.”
In summary, we learned that undocumented immigrants have tremendous need for behavioral health services for a variety of reasons that are more common for this group than other immigrant CHC patients.
Paradoxically, one interviewee noted that undocumented immigrants who lack a payer source could have easier access to behavioral health services because providers can be more flexible with offering medical and behavioral health on the same day. California’s same-day billing restrictions on medical and behavioral health for CHCs do not apply when there is no payer.
We heard that the current high rates of behavioral health use are the result of local and state government investments to address behavioral health need, including bringing in additional providers to address substance abuse. Our interviewees mostly discussed mental health needs among undocumented patients, though; there was relatively little discussion about treatment for substance use disorder (SUD). And despite the higher likelihood of having visits for behavioral health among undocumented patients, the reach of CHCs is limited. The resources and services clinics provide cannot meet the demand. We heard from one CHC that there has been a 60-to-90 day wait to get an appointment for behavioral health.
Telehealth Use among Undocumented Patients Is Comparable or Greater than among Medi-Cal Patients
Telehealth makes up around a quarter of study visits statewide and in LA County, which is striking since it was negligible prior to the pandemic.
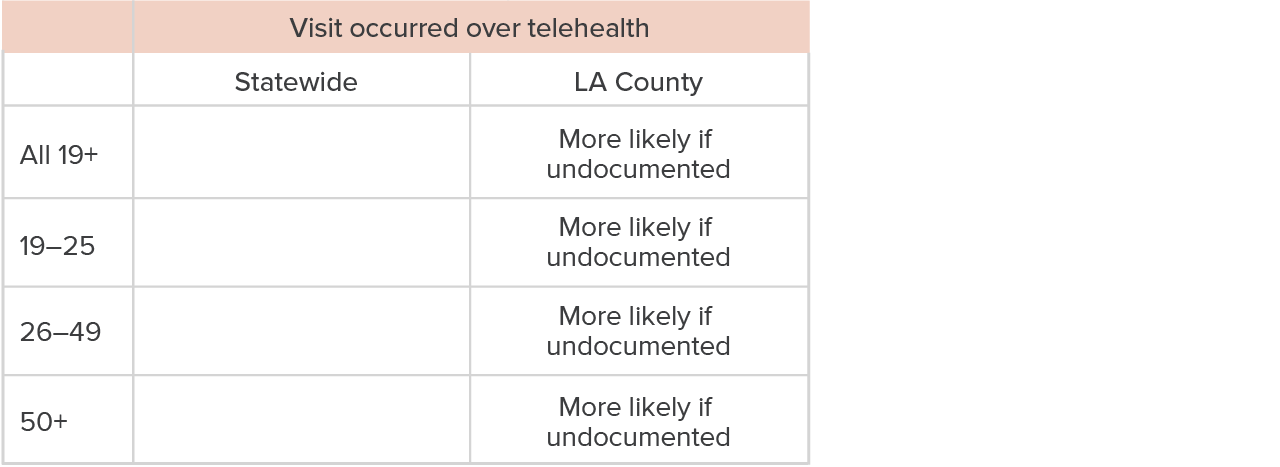
- Statewide, the likelihood of visits occurring over telehealth does not differ between undocumented patients and Medi-Cal patients (Table 9); this is consistent across our analyses of all adults and adults by age group (see Technical Appendix Tables B9 and B10).
- In LA, the likelihood of having visits over telehealth is slightly higher among undocumented patients compared to the Medi-Cal patients (Figure 9; Technical Appendix Tables B11 and B12). Being undocumented is associated with about a 5.6 percent increased likelihood of getting telehealth in LA, according to our adjusted analyses.
How undocumented status is associated with having a visit occur over telehealth
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s California and LA County community health centers.
NOTES: “More likely if undocumented” indicates that undocumented status is significantly associated with visits occurring over telehealth, and a blank box indicates no (significant) association. These characteristics describe regression-adjusted estimates in Technical Appendix Tables B9, B10, B11, and B12. The regressions are linear probability models of the likelihood of a visit occurring over telehealth with undocumented status. Control variables include age at visit, sex, race/ethnicity, preferred language, as well as fixed effects for county (clinic in LA County) and calendar year. Standard errors are clustered by county (clinic). Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
Undocumented patients in LA County used telehealth during the pandemic at slightly higher rates than Medi-Cal patients
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s LA County community health centers.
NOTE: Trends of annual percent of visits occurring over telehealth presented for undocumented and Medi-Cal patients at an OCHIN member community health center in Los Angeles County.
LA’s findings are especially interesting because the association is concentrated among mid- and older age groups of undocumented immigrants (Figure 10).
While almost a quarter of study visits in LA County are delivered via telehealth, relatively few individuals participate in these visits: less than 4 percent of study patients in LA (2,696 out of 70,299) ever use telehealth. An interviewee also noted that some patients and providers strongly prefer in-person visits for reasons that included the ability to assess patients’ health and talk through personal circumstances in person.
Visits for undocumented patients are more likely to occur over telehealth in LA County
SOURCE: ADVANCE network data for low-income patients ages 19 and older who are likely to be undocumented or who are enrolled in Medi-Cal and get care in OCHIN’s LA County community health centers.
NOTES: Bars represent regression-adjusted associations between visits being conducted over telehealth and patient undocumented status, scaled by mean outcome. Regressions are linear probability models of the likelihood of having a preventive care coded visit associated with undocumented status. See Technical Appendix Tables B11 and B12 for model estimates. Control variables include age on the day of the visit, sex, race/ethnicity, preferred language, as well as fixed effects for county clinic and calendar year. Standard errors are clustered by clinic. Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater.
*p<0.05 **p< 0.01
It is also notable that undocumented patients in LA, who are less likely to ever use telehealth, have higher shares of visits over telehealth than Medi-Cal patients. This implies that the undocumented patients who use telehealth are heavier users on average. Interviewees said that telehealth may help patients overcome logistical barriers to care, including transportation and scheduling visits around work, that may be more pronounced in the undocumented group. Telehealth can also be a way for undocumented immigrants to feel safe from COVID-19 and from immigration enforcement while receiving care.
- Older adults who are less mobile may use telehealth because they cannot come to appointments, although our telehealth users tended to be younger than non-users. On average, telehealth users are 40 years old, while non-users are around 44. Telehealth users are more likely to be white (or Native American/Alaska Native, though this is a small group and the difference reflects the actions of a few individuals). Telehealth users are also more likely to have English as their preferred language.
The higher representation of younger and English-speaking patients is consistent with comments from two of the experts we interviewed, who expressed concern that older and non-English-/non-Spanish-speaking patients would struggle to feel comfortable with the technology or would not know to request language services they are entitled to. A recent report based on the experiences of low-income telehealth users recommends integrating interpretation services and access to language-concordant providers to improve telehealth’s promise going forward (Joynt 2023).
Undocumented Older Adults and Medi-Cal Expansion
Although the final Medi-Cal expansion to all undocumented immigrants is not yet here, we can learn from other recent expansions. Statewide enrollment numbers followed different patterns for young adults and older adults. The pandemic makes it difficult to draw definitive conclusions about how different age groups of undocumented study members responded to becoming eligible for Medi-Cal, but we can describe some of the trends we find.
Statewide, enrollment rose at a steeper rate among older adults (30%) between the first and seventh months of their new eligibility than among young adults (12%, Figure 11). These differences are reflected in our CHC study data as well. The steeper response is not surprising, given the greater health needs of older adults and the fact their expansion did not coincide with the start of a public health emergency, as the young adult expansion had. Still, one takeaway is that people at the upper age range are likely to respond in greater numbers to the coming 26 to 49 expansion.
Older adults enrolled in full-scope Medi-Cal more rapidly than young adults
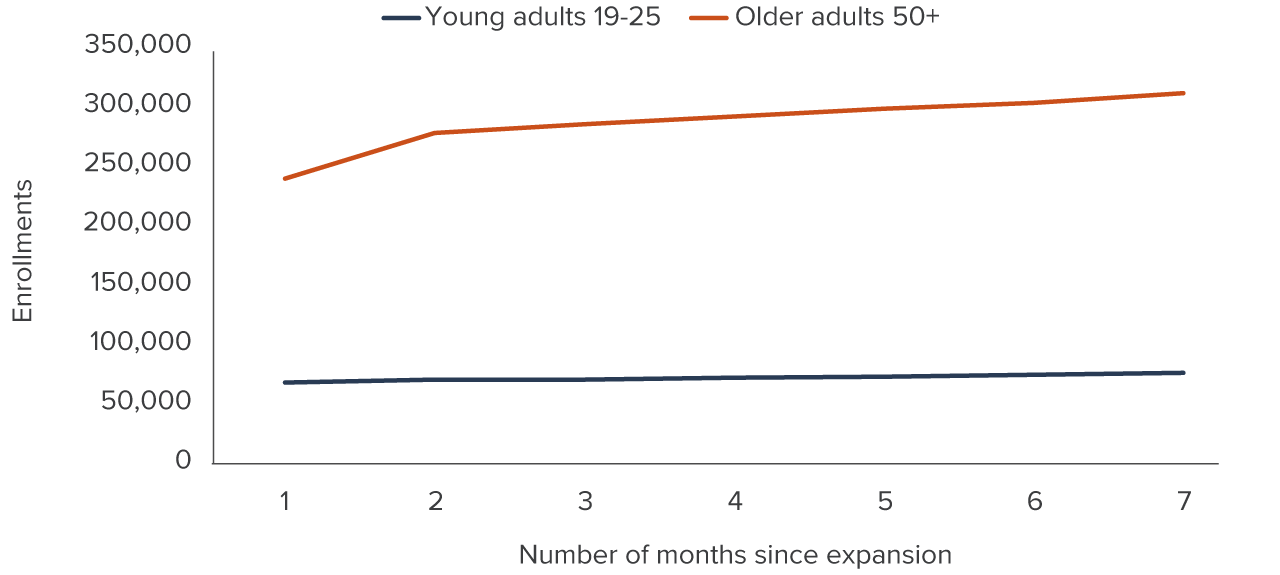
SOURCE: California Department of Health Care Services enrollment data, organized by the California Health Care Foundation.
NOTES: One month since expansion corresponds to mid-January 2020 for young adults, and mid-May 2022 for older adults. The COVID-19 pandemic affects the young adult trend beginning three months after expansion, and the entire trend for older adults.
In our CHC data, nothing suggests that Medi-Cal became a more prominent payer immediately following the 2020 expansion to young adults (see Technical Appendix C). Among older adults, the May 2022 Medi-Cal expansion shows a temporary increase in the share of people in this group getting care (Figure 12), while Medi-Cal group members showed no change. Together, these trends suggest that older adults are much more responsive to Medi-Cal expansion than younger adults; the coming 2024 expansion is likely to produce a temporary increase in visits for some in the 26-to-49 age group.
Older undocumented patients, but not undocumented young adults, increased visits following Medi-Cal expansion
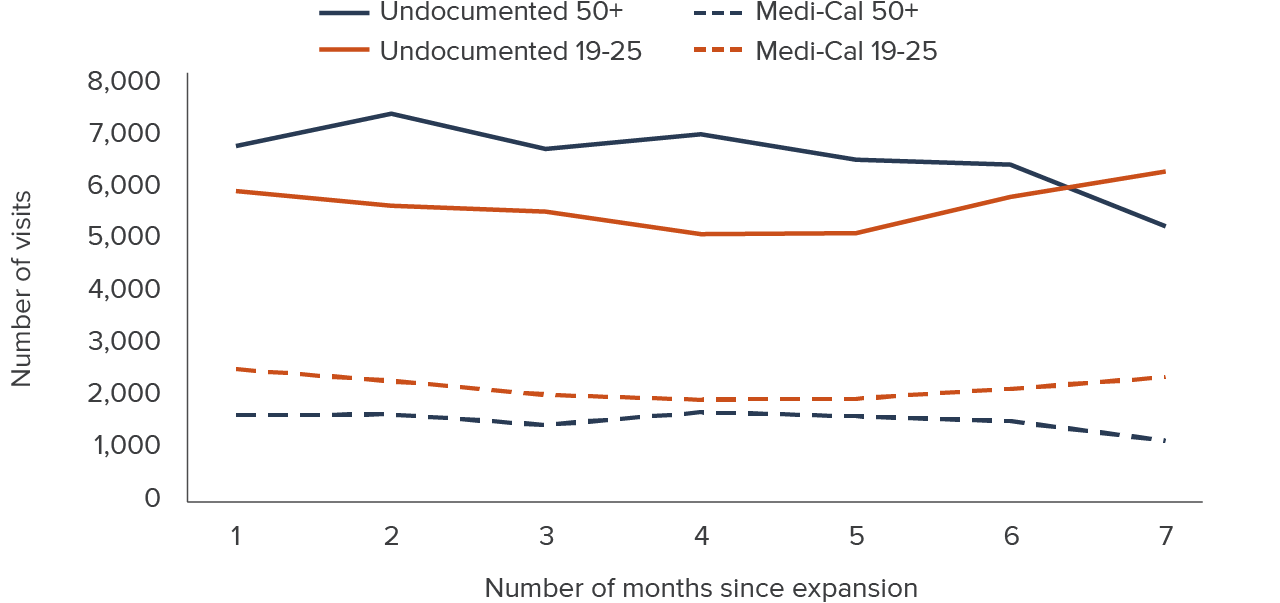
SOURCE: ADVANCE network electronic health records from OCHIN’s Los Angeles County community health centers, January–July 2020 and May–November 2022.
NOTES: Trends of visit volume presented for older adults ages 50+ as of May 1, 2022, and for young adults ages 26–49 as of January 1, 2020, who established care at an OCHIN member community health center in Los Angeles County between 2018 and 2020. The dates used for age definition correspond to the timing of Medi-Cal expansion to undocumented immigrants for that age group.
Barriers to Care for LA’s Undocumented Immigrants
Lack of insurance is part of how we identify undocumented patients, and it will be addressed by the 2024 Medi-Cal expansion, so we were especially interested in understanding other barriers. These barriers are multifaceted, spanning legal, financial, linguistic, and logistical difficulties that can override individuals’ intentions to access health care.
We used interviews to fill in the gaps on why some undocumented immigrants may not be getting care, or enough care, because our quantitative analyses can only speak to patients who are connected to health care. Our experts spoke specifically to the LA County context, but LA is a particularly welcoming and well-resourced county for immigrants, so some of the challenges they describe may be greater in other parts of the state. We periodically confirmed that the comments and stories the interviewees shared were specific to the undocumented experience, but some statements could refer to the broader immigrant community.
Fear and Confusion about Federal Immigration Policy Pose a Key Hurdle
The federal public-charge rule is a key barrier to accessing health care and other safety net resources, according to every expert we interviewed. The rule allows immigration officers to designate certain immigrants as a “public charge” based on their use of certain public benefits, a designation that may jeopardize an immigrant’s approval for an entry visa, admission to the United States, or later regularization to legal permanent residency (known as getting one’s “green card”). We heard from a number of experts that recent changes to the rule, described in Technical Appendix D, produced confusion and led immigrants to fear both Medi-Cal and My Health LA, though neither is connected to becoming a public charge (with the exception of long-term care such as nursing home care) (National Immigration Law Center and Protecting Immigrant Families Coalition 2022).
Interviewees related situations in which undocumented immigrants declined to enroll in safety net health programs they are eligible for, or asked to be removed if they are already enrolled.
One expert said, “[T]he federal [public-charge] rule had a chilling effect on people being willing to enroll in programs… They’re still showing up for care and saying, ‘No, just see me on a sliding scale.’”
Another reported “[My Health LA] participants… saying, ‘please just disenroll me because of the public-charge rule.’”
Limited Information and Misinformation Are Enduring Challenges
My Health LA provides access to health care for low-income uninsured, undocumented immigrants in Los Angeles County. According to our interviewees, the LA County region provides many resources for residents while there are limited resources for immigrants in rural areas outside the region. Immigrant enclaves and other community networks in Los Angeles County are sources of informal support and information for undocumented immigrants navigating the complex health system and social safety net programs.
Undocumented immigrants can receive important information about resources from promotoras (community health workers) or from groups like the Benefits Access for Immigrants Los Angeles (BAILA) Network, which provides enrollment support and legal advice to immigrants. We also heard that CHCs themselves do a lot of work enrolling patients into Medi-Cal, nutritional assistance, and other safety net benefits. Despite these community resources, lack of information was highlighted by many interviewees as a barrier to getting health care.
Lack of knowledge about the complex health system can lead people to forgo health care benefits through perceived legal barriers to care. Misinformation fills the vacuum left by a lack of access to legal resources that can respond to individuals’ concerns or questions. One example from an expert is when some notarios, or notaries, give incorrect information about safety net programs to undocumented immigrants who do not have more knowledgeable sources to turn to.
Pricey LA Imposes Financial Barriers to Care
The high cost of living in Los Angeles County poses great challenges for undocumented immigrants and low-income families. According to the California Poverty Measure, which accounts for geographical differences in housing costs, LA has the highest poverty rate (13.7%) among the state’s counties, 2 percentage points higher than the state average (11.7%) (Danielson, Malagon, and Bohn 2022).
High costs force individuals to prioritize their basic needs, forgoing health services that do not fit into their constrained budgets. In the words of one interviewee, “A lot of undocumented immigrants are low-wage workers. They don’t have extra fungible income. So, any income that they have often gets spent on housing, food, basic supplies, and their kids, so health care sometimes drops to the bottom of the list.”
Undocumented immigrants also worry about what will happen if they cannot afford to pay for health care after receiving it. Interviewees noted patients’ concerns about medical debt, Medi-Cal liens, and immigration sponsor deeming (in which immigrants must include their sponsor’s income in program applications—see National Immigration Law Center 2019), all of which pose barriers to signing up for safety net programs or getting health care. Low incomes can be a double-edged sword with respect to helping individuals access health care.
Health care safety net programs are targeted to low-income individuals—both Medi-Cal and My Health LA have an income eligibility threshold of $20,120 for a single person—but low-wage jobs themselves can stand in the way of getting health care. Undocumented immigrants with low-wage jobs tend to lack stable work schedules and paid time off, resulting in missing or delaying care. One interviewee noted that CHC visits outside normal work hours are coveted since they reduce conflict with patients’ jobs.
Transportation and Language Needs Pose Barriers in Multiple Ways
Undocumented immigrants may lack transportation to travel to health care providers. Transportation needs can also be the result of language needs, with patients having to travel long distances to see providers who speak their preferred language. Barriers can also stem from the lack of a cultural bridge, or an understanding and integration of cultural needs in health care.
Transportation barriers to care are present especially for older adults who are less mobile and may have greater health needs. One expert differentiated transportation access by residency tenure: long-settled immigrants are familiar with bus routes and know how to key in on specific phrases even if they do not necessarily speak English. More recent arrivals have a harder time navigating the sprawling county and its public transit system.
Complicating the picture further is LA’s high level of linguistic diversity. Most health care services and resources are provided in English or Spanish, while resources in Asian and Pacific Islander languages are not provided as often.
The Medi-Cal program provides a concrete example of the difficulties in serving expansive linguistic needs. The program establishes threshold languages by geography, and plans must provide materials in these languages to individuals who are not English-proficient. However, there are about 50 languages represented among our LA County study members and only a few, including English and Spanish, are threshold languages in LA. Technical Appendix E contains a complete list of LA County study patients’ preferred languages.
Furthermore, experts shared that patients may be unaware of their right to an interpreter and to receive materials in their preferred language as a result of the low health literacy among this group. Instead, older children and application assisters often serve as informal interpreters.
On a positive note, these barriers could be effectively addressed through staffing and other resources. We heard from several experts about the importance of hiring bi- and multilingual providers at CHCs, improving the availability of translation services, and providing document translation into a range of languages that go beyond LA’s 11 Medi-Cal threshold languages. Hiring staff with needed language skills may be harder for some roles. For example, it takes a very high level of fluency to conduct therapy in a second language, which poses a challenge for hiring behavioral health providers who speak multiple languages.
Addressing These Challenges Can Help with Medi-Cal Enrollment in 2024
We learned that community outreach is integral in LA County. CHC-based experts described their efforts to host informational workshops, and highlighted other groups doing similar work, such as the BAILA Network (Benefits Access for Immigrants Los Angeles 2023). CHCs go into the community and attend school events to engage with people who may be eligible for resources but need more information.
While LA County provides support to access these resources, some experts we spoke with expressed concerns about county staffing shortages and weaknesses in the county health system in addressing the needs of all patients. Some CHCs have difficulty enrolling their patients in Medi-Cal through county welfare agencies, with assisters waiting on hold for long periods. The county has no back-channel access for clinic assisters, so they get in line with everyone else who calls. Patients may be long gone by the time a phone connection is made, and the assister may not be successful in getting them on the phone to speak directly with the county, derailing the enrollment effort. Additionally, we heard that relationships between counties and community-based organizations (CBOs) could be improved and that the county could incorporate more on-the-ground feedback from CBOs to improve programs and outreach.
Even after the expansion, however, insurance challenges may continue for undocumented immigrants. Medi-Cal eligibility is not the same as enrollment. The application process is complex and enrollment assistance is instrumental for CHC patients. We heard that immigrants do not always understand the questions asked, and consequently, share incomplete information when applying for Medi-Cal. They may also experience instability in employment or county residency, complicating their ability to collect the required supporting documents. Here, too, language support will be needed. According to an interviewee, “[p]atients are willing to trust you and come to you to get [Medi-Cal] enrollment done when this kind of service or workshop is provided in their language by someone who knows where they are coming from.”
Confusion can persist, even among those who have managed to enroll in Medi-Cal. One expert shared that patients lack a solid understanding of their Medi-Cal coverage in terms of scope, provider networks, and medical group geographic limits. As a result, some patients do not understand why their preferred provider is out of their network.
Conclusion and Recommendations
California will soon complete its series of Medi-Cal expansions to all low-income residents, regardless of age or immigration status. Ahead of this final policy change, our project provides needed evidence about undocumented immigrants’ health needs and their patterns of getting health care in community health centers (CHCs).
We find that being undocumented is associated with a lower likelihood of having visits specifically for preventive care. A range of issues drive this difference, from patients’ immigration-related concerns to their insurance status. Undocumented immigrants who increase visits or newly establish care for the first time following Medi-Cal may have long-standing unmet health needs that were unaddressed due to lack of insurance. However, it is promising that undocumented patients who are already established at CHCs get certain types of preventive services—including cancer screenings and adult vaccinations—at rates comparable to or exceeding those of Medi-Cal patients.
The need for and use of behavioral health services were strong themes that emerged in our data analysis and in our interviews with experts in Los Angeles County. Undocumented status was associated with a higher likelihood of having visits for behavioral health care, a result that holds across types of behavioral health services, from counseling to care related to substance use disorders. We heard that demand for care is very strong among undocumented patients even as they face long wait times for appointments, and as CHCs face challenges with hiring fully bilingual providers who can offer counseling in Spanish or other languages.
Telehealth is helpful for connecting some groups of undocumented immigrants to health care. It solves many logistical problems that low-income patients experience, such as inflexible job schedules or transportation challenges. For undocumented patients, the perceived safety of not having to go in person to a CHC campus can alleviate concerns related to immigration enforcement.
Still, telehealth may not be reaching its full potential across all regions of the state or for all demographic groups. Undocumented status is associated with a higher likelihood of having telehealth visits in LA County, but not statewide, and the use of telehealth in LA County was concentrated among younger, English-speaking patients. Some groups may need additional supports to access telehealth, such as older adults who need help navigating the technology and patients who need health services in languages other than English and Spanish.
The higher likelihood of undocumented immigrants receiving certain preventive services was concentrated in LA County, suggesting that strengths or assets can be leveraged there. The state may be able to learn from LA’s past investments, such as the strategy to include undocumented immigrants in the county’s medical program, My Health LA.
The recent Medi-Cal expansions—one to young adults, the other to older adults—present contrasting examples of how newly eligible undocumented immigrants respond to policies. Medi-Cal did not appear to emerge as a more prominent payer when young adults visited CHCs after the expansion, but it did appear that way for older adults. And although our data do not allow us to see whether new older undocumented immigrants established care at CHCs, we see that the volume of already-established patients increased temporarily after Medi-Cal expanded to older adults. The final Medi-Cal expansion, which targets ages 26 to 49, seems likely to produce a range of responses, with adults at the younger end of this final group less likely to respond quickly and those at the older end more likely to seek care through Medi-Cal coverage soon after becoming eligible.
In light of these findings, county welfare departments, community health centers (CHCs), and immigrant-serving organizations can expect an increased volume of Medi-Cal applicants who will need access to enrollment assistance, including language services. Accurate sources of information will be crucial for newly eligible undocumented immigrants in 2024. CHCs should also expect an increased volume of clinic visits, even among established undocumented patients, which will likely include high demand for behavioral health services.
- To prepare for the coming increases in demand, clinics would benefit from resources to hire more staff, especially those who are bi- or multilingual.
- Expanding telehealth use may ease several barriers to care that undocumented immigrants face. Incorporating language services into telehealth is one way to expand the technology’s reach.
- Some adults will need technical help with telehealth: CHCs or community-based organizations could provide tutorials on videoconferencing technology to get more patients comfortable with the idea of telehealth.
California has committed to investing in further expansions to Medi-Cal and moving toward a unified health care financing system through the Department of Health Care Services, the Office of Health Care Affordability, and the Healthy California for All Commission. A stronger understanding of the health issues and patterns of care among undocumented immigrants today can help the state prepare for future health needs along with other challenges around accessing health care with the final Medi-Cal expansion.
Topics
Health & Safety NetLearn More

Covered California Boasts Nearly 2 Million Enrollees, with Some Dreamers Now Eligible

California’s Medi-Cal Expansion Is Lowering Poverty among Undocumented Immigrants

In First-in-Nation State Law, All Low-Income Residents Qualify for Medi-Cal

Video: Health Conditions and Health Care among California’s Undocumented Immigrants
Telehealth Usage among Low-income and Undocumented Californians

Low-income and Undocumented Californians Struggle with Mental Health