Table of Contents
- Key Takeaways
- Introduction
- How Are California’s Teens Faring?
- Accessing Mental Health Services Can Be Challenging
- Schools Are Promising Places of Intervention
- District Spending Has Increased but Gaps Remain
- Conclusion and Looking Ahead
- Notes and References
- Authors and Acknowledgments
- PPIC Board of Directors
- Copyright
Key Takeaways
Adolescence is a critical developmental period characterized by rapid physical, emotional, and cognitive changes that shape long-term health and well-being. Because roughly half of all lifetime mental health conditions emerge by age 14, early identification and intervention are essential. Currently about three in ten California children ages 12 to 17 report symptoms that meet the criteria for serious psychological distress over the past year.
To address this issue, California recently implemented two programs, the Children and Youth Behavioral Health Initiative (CYBHI) and the California Community Schools Partnership Program (CCSPP), which invest a combined $8 billion in the mental health of children and teens, including school-based services.
This report provides an up-to-date picture of teen distress, looks at school-based services, and reviews how districts are spending their money on student mental health. We find:
- One-third of students in our study report chronic sadness, and 14.5 percent suicidal thoughts. Teens of color—especially Native Hawaiian/Pacific Islander and multiracial students—report higher levels of distress than their white peers. →
- Girls report substantially worse mental health than boys. This gap emerges early and persists throughout high school. →
- Teens in rural schools have worse mental health. We find a gradient effect, with students in the most urban schools having better mental health than their counterparts in suburban, town-based, and rural schools. →
- Teens in the poorest schools are about 8 percentage points more likely to report chronic sadness/hopelessness compared to those in the richest schools. →
- Half of teens reporting a need for help from a counselor or therapist and who get help do so at school. However, teens have a strong preference to talk to someone they know rather than go to counseling. →
- Bolstered by the influx of federal and state pandemic recovery funds, school district per student health spending has nearly doubled in recent years. Between 2018–19 and 2023–24, total school district spending on health and mental health services in California rose from $934 million to $1.64 billion. Funds are mostly allocated to personnel costs. However, as the pandemic-related, one-time funds have expired and the state faces growing budget constraints, maintaining these expanded resources will be challenging. →
- District spending on mental health is similar for low- and high-poverty schools. And although school districts across geography—city, suburb, town, and rural—have increased spending, rural districts still lag behind their more urbanized counterparts. →
- We found lower suicidal thoughts but no relationship between chronic sadness among teens and two types of school-based supports—community schools grants and school-based health centers/wellness centers. These resources are only available in a subset of schools and do not capture the full universe of school-based mental health supports available. →
Introduction
Adolescence is a critical developmental period characterized by rapid physical, emotional, and cognitive changes that shape long-term health and well-being. Because roughly half of all lifetime mental health conditions emerge by age 14, early identification and intervention are essential (NIHCM Foundation 2024). Rates of depressive symptoms and suicidality have been rising since about 2009. The high rates of poor mental health observed in national data are also evident among California’s adolescents. About three in ten California children ages 12 to 17 reported symptoms that meet the criteria for serious psychological distress over the past year.
The COVID pandemic not only worsened this trend nationwide but also exposed longstanding inequities in both the prevalence of conditions and access to treatment (Jones et al. 2022). Some positive signs in 2023 (the most recent year of available data) suggest the pandemic-related uptick is abating, but levels are still high and a cause of great concern across the country and in California. Our work here informs policies to support teen mental wellness and lays essential groundwork for future evaluations of school-based mental health services.
Despite rising levels of need, adolescents across the US and in California face widespread challenges accessing mental health services (Lu et al. 2021; Xu et al. 2025). For families who pay out of pocket, cost alone can be prohibitive (Overhage et al. 2024). In California, the shortage of providers and their unequal distribution across different communities and regions are key barriers. Nevertheless, strong family and school connectedness during adolescence can have lasting protective effects on mental health, behavior, and overall well-being into adulthood (Gibb et al. 2019).
Teens spend most of their time at school, which makes it the ideal place to identify mental health needs and deliver services. School-based health centers (SBHCs) have been around for decades and primarily serve communities that face barriers to care. Typically, they are primary care clinics that do screenings, vaccinations, and acute care, but some also provide mental health care (Arenson et al. 2019). Even in the absence of SBHCs, schools have traditionally relied on core support staff—such as counselors, psychologists, and social workers—to serve struggling students. Teachers also play a key role by identifying and referring students in need of services (Hoover & Bostic 2021; Pan et al. 2023).
California has made recent major policy and funding commitments to expand school-based mental health systems as part of the governor’s Master Plan for Kids’ Mental Health. The Children and Youth Behavioral Health Initiative (CYBHI) is a five-year, $4.1 billion effort aimed at transforming the delivery of behavioral health services for children and youth in California. And the California Community Schools Partnership Program (CCSPP) invests $4.1 billion to support expanding community schools—which are schools rooted in relationships to the families and communities they serve—coordinating health, mental health, and pupil support services. Nevertheless, as one-time pandemic funding sources run dry and the state’s budget challenges mount, the sustainability of school-based mental health programs is at risk.
In this study we use two self-reported measures—having chronic sadness/hopelessness and having suicidal thoughts in the past year—from two different surveys of California public school students in grades 7, 9, and 11 to proxy for poor mental health and the need for services. To lay the groundwork, we first present a detailed overview of teens’ mental health outcomes reflected through age, gender, and race—refining these findings by school characteristics such as urbanicity and socioeconomic composition. Next, we examine the gaps between mental health needs and access to services, as well as what teens report about whom they prefer to talk to when they are feeling very sad. We then take a closer look at school-based supports like school-based health centers, wellness centers, and community school programs to explore how they relate to student need. Finally, we look at how district-level spending on student health varies by key district characteristics, highlighting changes from pre- to post-pandemic years. Where relevant, throughout our discussion we provide context and framework from national studies within which to understand California’s teens, the challenges they face, and solutions they need. We conclude with recommendations.
How Are California’s Teens Faring?
Adolescent rates of depressive symptoms and suicidality have been rising since about 2009 and increased dramatically during that period (Technical Appendix Figure A9). Moreover, several recent national studies have documented rising shares of adolescents reporting mental health problems (Coley et al. 2025; Mojtabai & Olfson 2020; Twenge et al. 2019). Although some positive signs in 2023 (the most recent year of available data) suggest the pandemic’s effect is abating, continuing high levels of poor adolescent mental health are still a cause of great concern.
These high national rates of poor mental health are also evident among California’s adolescents. About three in ten children ages 12 to 17 have recently reported symptoms that meet criteria for serious psychological distress according to a validated psychological measure over the past year (Figure 1). In general, girls reported much higher shares than boys (38% vs. 20%), as did older adolescents (15 to 17) than younger (12 to 14). Teens in lower-income families (below 200% of federal poverty or $62,000 for a family of 4) reported somewhat lower rates of serious psychological distress in the past year compared to those from higher-income families, though these differences are not statistically significant.
Three in ten California adolescents reported symptoms associated with serious psychological distress
Serious psychological distress, past year (%)

SOURCE: California Health Interview Survey, pooled adolescent sample 2022–2024.
NOTES: Serious psychological distress measured over the past year using the Kessler-6, a validated instrument with six questions that ask about the frequency and duration of symptoms during the past year to screen for psychological distress. Scores range from 0 to 24, and a score of 13 or higher indicates serious psychological distress. Differences are significant by gender and age groups but not poverty levels.
Moreover—as Figure 2 shows—more teens have committed suicide or been hospitalized for self-harm compared to pre-pandemic years. For both self-harm and suicide, boys’ trends have been relatively stable in recent years—but girls’ have worsened. Male adolescents have consistently higher suicide deaths than females, but that gap has narrowed since 2021. More boys than girls attempt or commit suicide. But girls’ recent substantially higher rates of emergency department visits for self-harm suggest more nonfatal suicide attempts (Technical Appendix Figures A7 and A8).
Rates of teen self-harm and suicide have fluctuated but remain higher than pre-pandemic years
% change since 2016

SOURCE: California Injury Data by California Department of Public Health, 2016–2023.
NOTES: The trends represent changes relative to 2016 levels for emergency department visits for self-harm and deaths by suicide. In 2016 there were 8,745 visits for self-harm and 127 deaths by suicide among teens aged 12 to 17.
We use two self-reported measures of having chronic sadness/hopelessness or having suicidal thoughts in the past year to proxy for poor mental health and the need for services using the CHKS core survey module. About one in three students reported chronic sadness and nearly one in seven reported suicidal thoughts between 2017–2024. We also look at the mental health patterns of different student groups to get a sense of which teens most often need services.
Although many California teens are still struggling, in recent years fewer among those participating in the survey have reported chronic sadness/hopelessness and suicidal ideation. Between the 2021–22 and 2023–24 school years, chronic sadness/hopelessness reports declined from 35 to 28 percent, and suicidal ideation from 15 to 11 percent (Figure 3). These declines are statistically significant and suggest some recovery from pandemic-era heightened distress. Still, with nearly three in ten students reporting chronic sadness/hopelessness and over one in ten reporting suicidal thoughts in 2023–24, the need for sustained mental health supports remains critical.
The share of teens reporting poor mental health has decreased significantly in recent years
Share of teens (%)

SOURCE: California Healthy Kids Survey, grades 7, 9, and 11 for school years 2021–22 and 2023–24.
NOTES: Bars represent the mean share of teen respondents who report chronic sadness/hopelessness or suicidal thoughts in the past 12 months. T-test comparing the share of students who report each of the two measures during the two school years shows a statistically significant difference (p<0.001).
Student Demographics and School Characteristics Affect Outcomes
Gender gaps emerge early and persist through high school
Boys report significantly lower levels of mental health distress than girls across both measures. Boys are around 8 percentage points less likely to report suicidal thoughts and nearly 19 percentage points less likely to report periods of sadness (Figure 4). These sizable gaps remain even after accounting for grade, race/ethnicity, school, and year (Technical Appendix Table A13).
Girls are far more likely to report poor mental health than boys
Share of teens (%)

SOURCE: California Healthy Kids Survey, grades 7, 9, and 11 for school years: 2017–18 to 2023–24.
NOTES: Bars represent the mean share of teens who report chronic sadness/hopelessness or suicidal thoughts in the past 12 months. T-test comparing the share of students who report chronic sadness/hopelessness by gender shows a statistically significant difference between boys and girls (p<0.001).
These gender disparities appear early in adolescence and remain large across grade levels (Technical Appendix Figures A1 and A2). Female students consistently report higher rates of sadness or hopelessness than their male peers across all grade levels. Based on regression-adjusted estimates, in grade 7, nearly 38 percent of female students are estimated to have experienced chronic sadness/hopelessness, compared to about 21 percent of male students. This gender gap persists in higher grades (Technical Appendix Figure A1). Rates of reporting sadness or hopelessness increase with grade level regardless of gender, suggesting that emotional distress is more common among older teens (Technical Appendix Table A12).
Similarly, across all grade levels, female students experience higher rates of suicidal ideation compared to male students. The largest gender gap appears in grade 7, where about 18 percent of girls are estimated to have had suicidal ideation compared to 9 percent of boys (Technical Appendix Figure A2), and narrows somewhat in later grades. This narrowing may reflect both developmental and environmental factors, such as maturing coping mechanisms, changing school or social environments, or different rates of help-seeking and reporting. Existing research shows that boys are less likely to express willingness to use mental health services and tend to have higher levels of stigma when compared to girls, which may contribute to increasing levels of distress with age (Chandra & Minkovitz 2006).
Gender gaps are consistent across all racial/ethnic groups
Across all racial and ethnic groups, we saw that girls are more likely than boys to report symptoms of poor mental health. In our adjusted analyses, 39 percent of white girls are estimated to report sadness or hopelessness in the past year, compared to 23 percent of white boys. Similar patterns appear for Latino, Asian, and Black students. The gender gap is even wider for Native Hawaiian/Pacific Islander (NH/PI), American Indian/Alaska Native (AI/AN), and students of multiple races, where about half of girls reported chronic sadness or hopelessness (Technical Appendix Figure A3). We saw comparable gender disparities in suicidal thoughts. In every racial/ethnic group, girls are significantly more likely than boys to say they experienced thoughts of suicide. An estimated 23 percent of AI/AN and NH/PI girls report suicidal ideation, highest among all groups (Technical Appendix Figure A4).
Teens of color report higher levels of distress than their white peers
On average, one-third of our study students had chronic sadness/hopelessness, and 14.5 percent had experienced suicidal thoughts. Chronic sadness is more common for teens of color than their white counterparts (Technical Appendix Figure A5). We found the largest differences for Native Hawaiian/Pacific Islander teens and teens of multiple races. Asian students are slightly less likely than their white peers to have experienced chronic sadness. We found no significant difference for Black students. All non-white race groups except Latino teens are more likely to have experienced suicidal thoughts than white teens (Technical Appendix Figure A6).
School characteristics that are key predictors of poor teen mental health can be used for targeting resources
Investments in students are often targeted to districts or schools, making it helpful to know when certain school-level characteristics are associated with greater student need. We find that school poverty and school urbanicity (whether it is in a city, suburb, town, or rural area) are important correlates of teen mental health. Teens attending the highest-poverty schools were about 8 percentage points more likely to report chronic sadness than teens in the lowest-poverty schools, translating to 24 percent higher than the study average, but poverty was not associated with suicidal thoughts—the more serious outcome (Technical Appendix Table A15).
In our study group, 35 percent of schools were in a city, 40 percent in suburbs, 9 percent in towns, and 16 percent in rural areas (these are in order of declining urbanicity and further explained in Technical Appendix C). We find that rural location is associated with a 2 percentage-point higher likelihood of chronic sadness (or 6% higher than average) and a 1.4 percentage-point higher likelihood of suicidal thoughts (or nearly 10% higher than average) (Figure 5). Among non-rural schools we find a gradient effect, with teens in city schools having better mental health than teens in suburban schools, and both groups faring better than teens attending schools in towns or rural areas. Our findings for towns were indistinguishable from rural locales (Technical Appendix Tables A19 and A23).
Teens in rural schools have increased likelihood of poor mental health
Increased likelihood (percentage points)

SOURCES: California Healthy Kids Survey, school years 2017–18 to 2023–24; US Department of Education data on school urbanicity.
NOTES: The excluded group is non-rural schools (i.e., city, suburban, and town). Bars represent regression-adjusted associations of geography categories against two mental health outcomes—having chronic sadness and having suicidal thoughts in the past year—while controlling for school year. Standard errors are clustered by school district. We use linear probability and interpret the estimates as percentage point (pp) changes in this figure. We also describe them as percentages (%) relative to average values in the text. On average in our study, 33.0 percent of teens report chronic sadness and 14.5 percent report suicidal thoughts. See Technical Appendix Tables A17 and A19 for details. Effects are considered significant if they differ from 0 at the 95-percent level of confidence or greater. ***p<0.001
While we cannot conclude that school characteristics cause poor mental health, our findings are consistent with many other studies—teens in rural settings experience higher levels of emotional distress than their peers in other areas. This highlights the importance of addressing long-standing barriers to mental health care in these communities. These barriers include geographic isolation, limited availability of providers and community resources, transportation challenges, high costs, insurance coverage limitations, and stigma surrounding mental health (Garbacz et al. 2022). Telehealth can help mitigate the barriers around geographic distance and transportation by facilitating remote access to mental health care when in-person visits are difficult, providing an important supplement to face-to-face care in underserved rural communities. Mental health needs are especially well-served through this medium since a physical exam is not necessarily part of the visit. California has invested in two new telehealth based mental health apps for children, youth, and their caregivers through the CYBHI (Kazura et al. 2025).
Accessing Mental Health Services Can Be Challenging
Despite rising levels of need, adolescents across the US and in California face widespread challenges accessing mental health services (Xu et al. 2025; Lu et al. 2021; Kataoka et al. 2002). For families who pay out of pocket, cost alone can be prohibitive (Overhage et al. 2024). In California, the shortage of providers and their unequal distribution across different communities and regions are key barriers. Figure 6 shows the CHIS survey results from 2005 to 2023. Since 2019, around 20 percent of California adolescents have reported they received counseling or therapy for mental health needs in the past year. Despite this recent growth in receiving services, the reported need has grown even more substantially, though it has begun to decline.
About one in five California adolescents received mental health services in recent years
Share of teens (%)
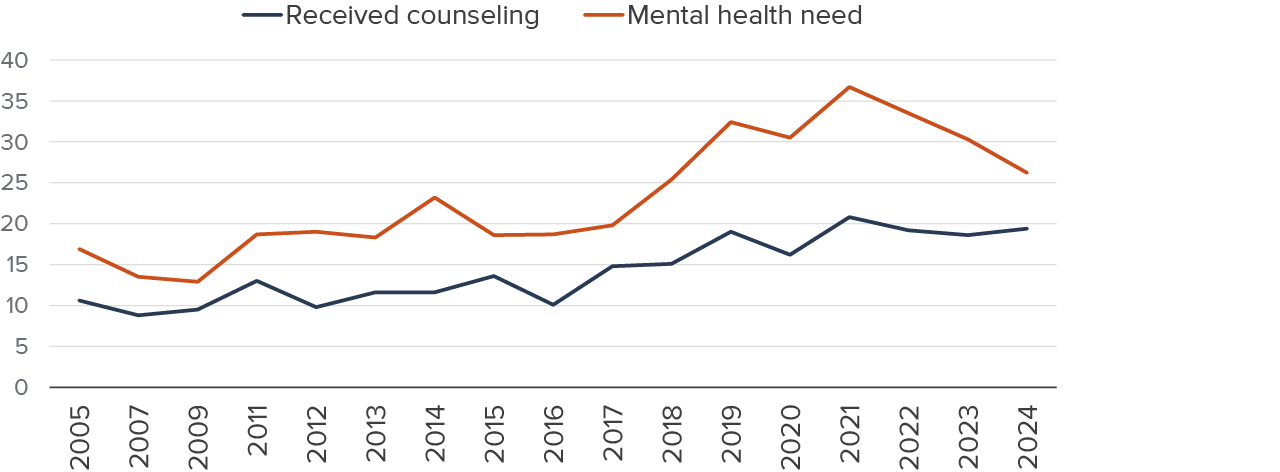
SOURCE: California Health Interview Survey, 2005–2024.
NOTE: Mental health need is identified by answering yes to the following question: “In the past 12 months did you think you needed help for emotional or mental health problems, such as feeling sad, anxious, or nervous?”
Which Teens Experience Service Gaps?
National-level research has documented disparities in access to mental health services across income, race/ethnicity, geography, and insurance status. Generally, Black, Hispanic, and Asian teens with depression are less likely than their white peers to receive mental health services. Moreover, Black youth are more likely to rely on emergency departments—suggesting limited access to outpatient care (Lu et al. 2021). Cultural beliefs and stigma related to emotional distress and mistrust in healthcare systems can make teens from some racial and ethnic minority groups and their families more hesitant to seek mental health services (Ma et al. 2025; Zhou et al. 2025). LGBTQ adolescents also experience higher rates of mental and behavioral health conditions and face significant barriers to accessing services (Hoffmann et al. 2022).
In California we see similar patterns across demographic groups. Girls and older teens (ages 15–17) report the highest levels of mental health need (about 45% and 40%, respectively) and have the largest gaps for receiving counseling (Figure 7). Boys and younger adolescents (ages 12–14) report lower mental health needs, and while gaps between need and service are smaller, they are still present. Adolescents from low-income families report lower mental health needs and receipt of services than those in higher-income families, however the gap is similar between the two groups.
Girls and older adolescents report larger gaps between needing and receiving counseling
Percent

SOURCE: California Health Interview Survey, pooled adolescent sample 2022–2024.
NOTES: Mental health need is based on an affirmative response to the following question: “In the past 12 months did you think you needed help for emotional or mental health problems, such as feeling sad, anxious, or nervous?” Received services is based on an affirmative response to the following question: “In the past 12 months, have you received any psychological or emotional counseling?”
We analyzed detailed behavioral health questions from a subset of our study group in the 2023–24 school year from the CHKS and factors associated with whether students reported receiving help from a counselor or therapist when they needed it. Although teens of color were generally less likely to report receiving help than their white peers, the differences between white and Black or American Indian/Alaska Native were not statistically significant. Boys were 2.5 percentage points less likely than girls to receive help when needed. Students attending schools with a higher share of low-income students were slightly less likely to receive help. We did not see significant differences by grade level or by whether a school was located in an urban or rural area.
Digging Deeper into Where Teens Turn for Help
Teens are in a life stage where they need to individuate from the adults in their lives and forge their own identities, but the subset who participated in the 2023–24 CHKS behavioral health module recognize the important roles that adults can play in emotionally difficult times. A majority of respondents (70%) said that talking to an adult could help a hypothetical peer feel better if the teen were having a hard time and feeling very sad, stressed, lonely, or depressed. A similar percent (67%) said that they know where to go or who to contact at school when they themselves feel this way. The people most frequently identified as resources to talk to are friends (64%), parents (56%), a counselor or therapist (23%), and a teacher or another adult from school (22%). Around a fifth (19%) reported that they would be afraid to get help and 24 percent said they would not know what to do (Figure 8).
It is not surprising that teens are much more likely to turn to friends or family than to a counselor or therapist when they feel stressed. Yet the much lower preference for professional help highlights challenges around trust, stigma, and mental health literacy. Schools and communities may need to do more to clearly communicate available services, normalize their use, and build confidence in them. Innovative approaches, such as peer-to-peer support programs in schools, offer promising models for meeting teens where they are.
Most teens identify friends and parents as people to speak to when they feel very sad
Percent

SOURCE: California Healthy Kids Survey Behavioral Health Module, 2023–24 academic year.
NOTES: Includes teens from grades 7, 9, and 11 in schools that participated in the Behavioral Health Module. Analysis limited to teens who responded to key behavioral health questions (see Technical Appendix A for details). Teens were asked to identify who they would speak to if they were feeling very sad, stressed, lonely, or depressed. Percentages sum to more than 100 because teens could select as many answers as applied. About 1,700 teens did not respond to this question, and percentages are calculated among respondents only (N=92,497).
School may well be the best location for teens to connect with friends, counselors, and therapists, in addition to teachers. Schools often serve as an accessible place for students to seek support for their mental health needs. Around 44 percent of teens who said they needed help from a counselor or a therapist in the previous year received help and about half of those who received counseling and therapy services got it at school (Technical Appendix Table A25). Schools can help fill gaps and address barriers in accessing mental health services like provider shortages, stigma, lack of transportation and knowledge of where to access services.
Schools Are Promising Places of Intervention
California has made large investments in recent years to bolster school-based resources for mental health and well-being. Both the California Department of Education and the California Department of Health Care Services have targeted initiatives and investments to support schools in expanding the role they play in providing mental health services to students (Technical Appendix B).
Since schools are readily accessible to youth and families, they have been an access point for health services and have increasingly been involved in promoting wellness (Shelton & Owens 2021). Embedding services directly into the school environment has proven to be an effective way to increase access and meet students where they are (Golberstein et al. 2024). Moreover, early intervention and treatment in schools have been shown to reduce mental illness and have been linked to some improvement in academic outcomes (Hoover & Bostic 2021). As awareness grows around the connection between mental health and academic success, schools are increasingly embracing integrated mental health supports as a strategy to foster well-being and improve educational outcomes (Hoover & Bostic 2021). Many implement universal programs to improve student mental health.
Schools address a wide range of mental health concerns, including stress, anxiety, depression, bullying, family issues, and substance use. Students often seek help for problems related to school, friends, or home. According to national survey data, just over one-third of adolescents receiving mental health care—especially those with public insurance, from low-income families, or from racial/ethnic minority groups—do so exclusively through schools (Ali et al. 2019). And for those with high mental health needs or specific diagnoses, school-based mental health services account for the largest single share of service use compared to other settings (Duong et al. 2021). However, for more serious conditions like suicidal ideation or diagnosed disorders, students are less likely to rely solely on school-based treatment and often receive services in combination with other outpatient mental health providers (Ali et al. 2019).
School-based mental health services can include a broad range of interventions—from universal supports like screenings and social-emotional learning programs to targeted and intensive services such as therapy, crisis intervention, and medication management (Technical Appendix B). Services may be provided exclusively by outside community providers or by school or district personnel—sometimes in combination with outside providers. Public schools typically employ various mental health professionals, including school counselors, psychologists, social workers, and nurses. According to national data, 84 percent of public schools provide individual-based interventions such as one-on-one counseling or therapy, 70 percent offer case management to help coordinate services, and 66 percent make referrals to external mental health providers when needed (Pan et al. 2023).
In a 2021–22 statewide survey of 1,347 California school administrators, most respondents (93%) reported that their school implemented at least one program to improve student mental health—social-emotional learning curricula and Positive Behavior Intervention and Supports being the most common (CDE & UCSF 2022). These types of programs have shown positive effects on student academic, emotional, and behavioral outcomes (Bradshaw et al. 2012; Greenberg 2023).
Some Schools Have More Targeted Resources to Support Student Mental Health
School-based health centers (SBHCs), school wellness centers, and community schools are examples of specific investments and programs that are well-positioned to provide structured school-based mental health programs to California adolescents in public schools. These specific services, however, represent only a small subset of the supports available in schools. Even in the absence of these specific resources, many schools have school-based professionals such as psychologists, counselors, and school nurses who provide mental health services. In this section, we analyze how these resources are distributed across California public schools relative to potential need based on poverty (proxied by percent of students eligible for free or reduced-price lunch, or FRPM) and urbanicity, and describe how these investments correlate with mental health outcomes. We focus on poverty and urbanicity because these characteristics are readily observable and also factor into things like school funding formulas, making them practical levers for targeting resources, and because our earlier findings show that teens in high-poverty and rural schools report worse mental health outcomes.
Community schools
Community schools represent a “whole child” school improvement strategy, where educational institutions collaborate closely with teachers, students, families, and community partners to align resources and enhance student outcomes (California Department of Education 2024). Well-implemented community schools help in improving student outcomes (Swain et al. 2025) and developing a positive school climate, which is associated with positive student mental health outcomes (Germain and Klevan 2025).
The California Community Schools Partnership Program (CCSPP) is a major initiative, allocating $4.1 billion to provide significant funding to enhance and expand community school models. CCSPP implementation grants for community schools began in 2021–2022 and were expanded to 1,468 schools by 2023–2024. These grants serve districts with a large percentage of high-need students or those with higher-than-state-average dropout, suspension, or expulsion rates. In total, an estimated 800,000 students are in schools that received the grants (Technical Appendix Table A31); nearly all are in high-poverty schools and around 83 percent are in cities and suburban areas (Figure 9).
The 2022–23 progress report for the initial CCSPP cohort found that participating schools improved their capacity to support student mental health by increasing clinician staff and fostering school environments that normalize conversations about mental health (Boal et al. 2023).
School-based health centers and wellness centers
School-based health centers (SBHCs) and wellness centers (WCs) are clinics or other physical spaces located on or near school campuses that offer students a range of health services. Around 400,000 of California’s 5.8 million students attend schools with SBHCs/WCs; 72 percent of these students are in high-poverty schools and 92 percent attend schools in cities and suburban areas (Figure 9). Out of the 365 SBHCs and WCs, 296 offer mental health services.
SBHCs typically provide primary care, mental health counseling, and other services such as dental care, optometry, and health education. They play a key role in reducing barriers to care such as stigma, cost, transportation, and limited provider availability. Evidence suggests that SBHCs can help reduce disparities in mental health care by serving diverse populations—including gender-diverse, LGBTQ+, and students of color (Soleimanpour et al. 2024). Wellness centers primarily focus on behavioral health services.
Community schools and school-based health centers/wellness centers are concentrated in higher-poverty schools
Share of students (%)

SOURCES: Census Day enrollment data, CDE school year 2023–24; Free or Reduced-Price Meal (Student Poverty) data, 2023–24; National Center for Education Statistics (NCES) locale classification (additional details in Technical Appendix C); List of school-based health centers/wellness centers by California School-based Health Alliance; CCSPP implementation grant recipients cohorts 1,2 and 3 (2021–24).
NOTES: High-poverty schools are defined using a cutoff of 55 percent of students receiving free or reduced-price lunch, as this is similar to how the Local Control Funding Formula designates districts to receive additional funding. Data does not include non-traditional schools and some independently reporting charter schools. Counts of schools and enrollments can be found in Technical Appendix Tables A29, A30 and A31.
School-based health centers providing mental health services and community schools are associated with reduced suicidal thoughts
Because SBHCs/WCs and community school grantees are uniquely positioned to provide mental health services to adolescents, we conducted a focused analysis of schools that have these support structures and describe how these investments correlate with mental health outcomes. SBHCs/WCs that provide behavioral health services are associated with a 0.9 percentage point lower rate of suicidal thoughts—about 6 percent lower than the study average (Technical Appendix Table A33). However, we did not see any association with the chronic sadness outcome. SBHCs in California are often located at schools that rank higher on indicators of socioeconomic disadvantage and poor health outcomes (California School-Based Health Alliance, 2025), and this is likely to bias our study away from finding significant associations.
We find no association between attending a school with a community schools grant and experiencing chronic sadness, but a 0.8 percentage point lower rate of suicidal thoughts—5.5 percent lower than the study average (Technical Appendix Table A34). However, it is worth noting that community school grants are a relatively new investment and it may be too soon to fully assess the longer-term impacts of these investments on student mental health. They predominantly serve high-poverty schools (Figure 9) and given our finding that schools with higher poverty have greater mental health needs, these schools may have started from a higher baseline risk of poor mental health outcomes.
District Spending Has Increased but Gaps Remain
California’s K–12 school districts have expanded their investments in student health, including mental health services in recent years, bolstered by an influx of federal and state pandemic recovery funds. In this section, we compare unified and high school district health spending for the 2018–19 school year (pre-pandemic) and 2023–24 (most recent data). These expenditures reflect a range of supports for the general student population—including spending on counselors, psychologists, social workers, and school nurses among others.
Most Spending Goes for Personnel
Staffing remains a critical issue in California’s school mental health landscape. In 2019, student-to-support personnel ratios in California were high and fell short of recommendations from professional organizations (Technical Appendix Table C15). Unfortunately, this is the most current state data available that provides detailed, comprehensive information on the type of personnel employed at California schools. According to national statistics, in 2021 only 60 percent of California public schools employed at least one full-time equivalent (FTE) school counselor—well below the national average of 76 percent (US Department of Education, Office for Civil Rights n.d.). However, during and after the pandemic, schools directed a substantial portion of their mental health funding toward hiring additional staff. By 2023–24, California’s student-to-school psychologist ratio improved from 1,041 to 777 students per psychologist. California has invested in a workforce initiative to expand school-based mental health capacity by training and deploying wellness coaches, a newly certified, non-clinical role that supports youth mental health and well-being.
Between 2018–19 and 2023–24, total school district spending on health and mental health services in California rose by 75 percent—from approximately $934 million to $1.64 billion. The majority of these expenditures— increasing from $840 million to $1.43 billion—continued to support personnel-related costs such as salaries and benefits for school psychologists, counselors, nurses, and other staff (Figure 10). Since a large share of the increased spending on health and mental health services in 2023–24 came from pandemic relief funds, the expiration of these grants is likely to jeopardize schools’ ability to sustain the increased investments schools made on staffing.
Expenditures on health and mental health increased 75 percent between 2018–19 and 2023–24 school years
District spending ($billions)

SOURCE: School District Annual Financial Data, 2018–19 and 2023–24.
NOTES: Bars represent statewide total district spending on health services and psychological services (excluding expenditures for special education). Includes unified and high school districts.
These spending increases likely reflect both rising student health needs during the pandemic and the availability of pandemic relief funds that enabled many districts—particularly those with fewer resources—to expand services (Lafortune et al. 2023). For example, between 2018–19 and 2023–24, pandemic relief funds like Elementary and Secondary School Emergency Relief and Expanded Learning Opportunities Grant funds comprised about half of the increase in average per student health expenditures (Technical Appendix Table C8).
Unified districts, which serve more than two-thirds of students in the state, report substantially higher per student health-related expenditures compared to high school districts. In unified school districts, per student expenditures on health and mental health services rose by more than 70 percent—from about $215 to $370 on average. This pattern could be due to greater administrative capacity, flexibility, or readiness to expand health services when additional funding became available during this period. These districts had the highest per student spending in both years. High school districts actually saw an even larger increase (about 85%) in health spending between the 2018–19 and 2023–24 school years, though per student remained lower (about $285) compared to unified districts (Figure 11).
Per student spending on health services increased considerably in the 2023–24 school year
Health expenditures per student

SOURCE: California Department of Education, SACS data and district enrollment data.
NOTES: Per student expenditures are calculated for each district by dividing the combined expenditures on health services and psychological services (excluding expenditures for special education students) by the total student enrollment in the district. Average expenditures are weighted by district student enrollment.
Rural districts spend the least despite higher student need
As our analysis above showed, teens in rural schools reported higher levels of mental health needs compared to those in more urban and suburban locations. While health expenditures increased across all geography types between 2018–19 and 2023–24, spending per student at rural school districts remained more than $150 lower than suburban and city districts despite higher student need (Figure 12). Districts located in urban cities reported the highest per student spending, rising from about $235 to $400 during this period (Figure 12).
Rural districts’ lower spending levels are likely related to limited capacity in terms of available providers, in particular mental health providers, which are much more limited in more rural regions of the state.
Districts in rural areas report lower spending on student-related health services
Health expenditures per student

SOURCES: School District Annual Financial Data, 2018–19 and 2023–24; California Department of Education district enrollment data, year 2022–23.
NOTES: Per student expenditures are calculated for each district by dividing the combined expenditures on health services and psychological services (excluding expenditures for special education students) by the total student enrollment in the district. Average expenditures are weighted by district student enrollment. Number of districts and share of students in each locale type can be found in Technical Appendix Table C9.
Significantly lower levels of health spending among rural districts remained even after we controlled for differences in student body enrollment size, poverty levels, and racial/ethnic composition. In contrast, patterns are not clear when we look by poverty level of the district. High school districts with more low-income students spent slightly less on health services in 2018, but by the 2023–24 school year this pattern had disappeared and showed no clear relationship (Technical Appendix Figures C1–C4).
Conclusion and Looking Ahead
Teen mental health challenges in California appear to have peaked during the pandemic and show signs of improvement since. Still, about three in ten adolescents in the state struggle with symptoms related to depression and anxiety and more than one in ten report they seriously considered suicide in the past year. Some groups have more difficulties than others. Girls report substantially worse mental health than boys. And teens of color—especially Native Hawaiian/Pacific Islander and multiracial students—report higher levels of distress than white teens. Teens attending schools in rural areas of the state consistently report higher rates of chronic sadness and suicidal thoughts, as do students attending schools with more low-income students. Telehealth could be a cost-effective way to bring services into isolated and under-resourced schools in rural areas.
Significant gaps exist between reported need for mental health care and receipt of services—especially for girls and older adolescents. Provider shortages, high costs, and transportation issues are all challenges to receiving care. Reaching teens at schools can address some of these barriers, which supports the increased focus and funding towards school-based mental health services. Schools are also an ideal place to deploy prevention measures to a broad group of teens. At the same time, reluctance to access professional help also highlights challenges around trust, stigma, and mental health literacy; schools may need to do more to clearly communicate available services, normalize their use, and build confidence in the community. Innovative approaches—such as peer-to-peer support programs in schools—offer promising models for meeting teens where they are.
When we look at schools with dedicated resources to address student mental health, we do find associations linked to lower rates of suicidal thoughts but no relationship with reports of chronic sadness. These findings should be interpreted in the context of where these resources are located: they tend to be more concentrated in higher-need communities, which could impact our results. It is also the case that initiatives like community schools and wellness centers are relatively new and more research is needed to evaluate their impacts.
Expenditures on health and mental health services by school districts have increased considerably in recent years. However, despite increased spending, districts in rural areas continue to lag behind even though students in rural schools report higher rates of mental health needs. In addition, over half of the increased spending on health-related services came from pandemic relief grants that have now ended, raising questions about whether schools will be able to maintain services. The state continues to provide funding for broad school-based mental health through programs like community schools, and there are continuing efforts to increase insurance coverage for school-based services through the Multi-Payer Fee Schedule under the California Youth Behavioral Health Initiative.
Moving forward, more up-to-date information is needed to help guide allocation of resources toward schools with higher mental health needs and where access and funding gaps are most pronounced. In particular, comprehensive school-level data on health and mental health personnel like counselors, psychologists, and other professionals would go a long way towards targeting more support to schools with fewer resources. Schools and districts will also likely need continued technical assistance to conduct medical billing at scale. Beyond the loss of pandemic funds, many California schools face financial challenges related to declining enrollments, which underscores the importance of leveraging additional funding sources.
Documenting the range of mental health services available in school-based clinics/wellness centers and through community school grants will be an important part of understanding what students are experiencing on their campuses. Further, continuing to evaluate California’s historic investment in teen mental health through California Youth Behavioral Health Initiative and community school grants will be important to refine strategies for effectively addressing students’ mental health needs.
Topics
Health & Safety Net K–12 Education Poverty & InequalityLearn More

Testimony: Teen Mental Health and School-based Support

How California Is Investing in School-Based Mental Health Services for Teens

Investing in Schools to Address COVID-19’s Toll on Youth Mental Health

Emotional Distress and Limited Access to Care Put Families’ Health at Risk

Pandemic or Not, Teen Mental Health Is Fragile