Table of Contents
- Key Takeaways
- Introduction
- Health Training Pathways’ Economic Returns
- Health Training Providers and Costs
- Who Pursues Different Health Programs at Community Colleges?
- Barriers to Improving Economic Opportunity via Health Training Pathways
- Conclusion
- Notes and References
- Authors and Acknowledgments
- PPIC Board of Directors
- Copyright
Key Takeaways
California’s health care sector is the largest and fastest growing in terms of employment. Many health care occupations do not require a four-year degree. They offer opportunities to those with some college for well-paying jobs that are available across most regions. In this report we provide an overview of the economic returns from community college health training programs and current information on enrollments across different programs and providers. It can help guide policy decisions and strategies for broader access to health careers with potential to increase economic mobility. We find:
- Intensive health training programs that result in associate degrees offer high economic returns. Registered nursing, dental hygienist, and a few allied tech programs nearly double earnings levels in the six years after people finish their degree. These occupations have wage levels well above average across most regions of the state. →
- Mid-length health programs resulting in certificates that take one to two years to complete—such as licensed vocational nursing and psychiatric technicians—can also lead to better-paying jobs. However, job opportunities and wage levels vary across regions. →
- Shorter-term health training that leads to positions such as nursing and medical assistants do not tend to confer significant wage gains. They can provide opportunities to enter the health care field and then complete additional education and training to access higher wage jobs. However, few people seem to take advantage of these stepping stones on a career pathway to higher-paying jobs. →
- Community colleges are the primary public provider of training and education for health care jobs. Women comprise most health program enrollments and there are also differences in program enrollments across racial/ethnic and age groups. →
- For-profit colleges also offer training programs for health jobs that require some postsecondary training. More than 60 percent of sub-baccalaureate health awards completed at California higher education institutions were conferred by for-profits. →
- Training providers we spoke with said that high demand from local employers and health credentials with clear job opportunities make connecting people to jobs much easier. They also articulate difficulties for those considering training: access issues and long waits for high-return programs because of capacity constraints, along with financial and family considerations.
Introduction
Health care is one of the largest and fastest-growing sectors in California’s economy due to a growing older adult population and health coverage expansions. Several jobs in the health sector offer relatively high wages and economic mobility for workers with some college training but no four-year degree. This is relatively unique in the labor market. The state invests a considerable amount in health workforce education and training—which in turn can expand routes to promising careers for more Californians.
Most state investments in health care training—and those aimed at broadening access to them—occur within the community college system, which is the primary focus of this report. For-profit institutions and community-based nonprofits also play a key role in training Californians for health care occupations. Comprehensive information from these providers is lacking, but to shed as much light on the broader training ecosystem as possible, we examine available data. The California Community College Chancellor’s Office (CCCCO) recently updated their Vision 2030 plan, which recommits to promoting economic mobility and specifically calls for expanded access to health care pathway programs. The Governor’s recent Master Plan on Career Education also calls for strengthening training pathways that lead to well-paying jobs in key sectors including health care.
The specific health programs Californians pursue have clear implications for future economic gains and career opportunities. Some of these training pathways—in particular programs that lead to an associate degree in nursing or radiologic technology—afford high earnings potential. But they can be challenging to access due to prerequisite course requirements, capacity constraints, and high costs. Still other programs—typically shorter ones such as nursing or medical assistants—do not tend to translate into sizeable earnings gains. With additional training these can be stepping stones along a career pathway, but relatively few people who complete them go on to complete longer, more intensive programs that would significantly improve their economic trajectories, at least not through the community colleges.
The substantial differences in choices across demographic groups—gender, age, and race/ethnicity—affects the extent to which Californians access earnings gains from health training programs. Gaps in information about promising health careers and access to training programs may limit some Californians’ pathways. Challenges to completing programs and differences in regional job opportunities and wage levels also impact the potential of health training to improve economic trajectories.
In this report, we present an overview of job opportunities and earnings potential for people who complete community college health training programs for occupations that do not require a bachelor’s degree. While programs vary in their value, many health credentials are notable for increasing economic gains—and some offer “stackable pathways” that build credentials and career opportunities over time. We analyzed quantitative data and conducted interviews with health training providers to learn more about the opportunities and barriers to health training programs. Here we synthesize the research to provide updated information on who is pursuing which health pathways in California and discuss strategies for improving access to health careers that can advance economic mobility. This information is critical for policymakers as they weigh health program pathway expansions and investments, and for community college practitioners as they make decisions about program offerings and guide students (and potential students) towards available training.
First, we provide an overview of the economic returns from completing different health training programs at the community colleges. Next, we describe health care training providers and costs. We then examine who pursues and completes different types of health training, with a focus on differences across demographic groups and the distribution of training programs across the state’s regions. Finally, we examine barriers that might explain these patterns. Throughout, we include insights from providers who work to connect Californians with health training and jobs.
Health Training Pathways’ Economic Returns
The largest community college health care training programs comprise four broad pathways. These represent the bulk (80%) of health care jobs that typically require some training beyond high school but less than a four-year college degree. They are:
- Nursing and medical assistants: registered nursing (RN), licensed vocational nursing (LVN), certified nursing assistants (CNA), and medical assistants
- Dental: dental assistants and dental hygienists
- Behavioral health: psychiatric technicians, alcohol and substance use counselors
- Allied and technical: Radiologic technology, pharmacy technicians, respiratory care therapists, paramedics, and emergency medicine technicians (EMT)
This group of health occupations is projected to grow at higher rates than overall job growth in the state, have job opportunities across all regions, and in most cases pay wages at least on par with median economy-wide levels—and in many cases well above. Other training providers, including for-profit institutions and nonprofit workforce agencies do prepare people for some of these occupations, but their program offerings tend to be limited to a few specific occupations, which we explore in a later section of the report.
Several of these pathways have opportunities to stack credentials—i.e., to complete shorter training programs and enter the workforce, then return later to complete additional training along a career pathway. For example, nursing pathways have a clear series of progressively longer training options that lead to registered nursing degrees and beyond. Similarly, dental assistants can pursue additional specializations and/or advance with more training to become hygienists (Bohn et al. 2016b).
Table 1 provides an overview of the occupations organized according to the intensity of training and education required, which aligns closely with their labor market value. The “High” category refers to occupations that require at least an associate degree and usually take several years to complete prerequisites, program requirements, and on-the-job training in clinical placements. Occupations in this category also have high wages relative to other labor market opportunities. The “Medium” category refers to health jobs that typically require long-term certificates that take between one and two years to complete, while the “Low” category includes jobs that require relatively short-term training (three months to one year) and have lower wage levels.
Registered nurses are the single largest occupation in the overall health care sector; more than 325,000 registered nurses work in California and more than 500,000 people have an active nursing license allowing them to work in the state. It is also the highest-paid profession among those we include in this report. As Table 1 indicates, many registered nurses enter the profession with a bachelor’s degree, which contributes to the overall higher wages. In California, just over half (54%) of registered nurses enter the workforce with a bachelor’s degree in nursing (BSN). Still, nearly four in ten (38%) start their nursing careers with an associate degree in nursing (ADN), which is sufficient to take the licensing exam and be qualified to work as a registered nurse. There are several programs—including online—that allow licensed registered nurses with an ADN to earn a bachelor’s degree in nursing (BSN) in a relatively short time.



Other occupations in the High category perform diagnostic testing and coordinate medical and dental care for patients. Occupations in the Medium and Low categories also provide direct care for patients, and some provide administrative support and may perform diagnostic tests. Most also require occupational licenses overseen by state boards responsible for creating training standards, certifying providers, and managing license test requirements. A few occupations do not require a state license—including medical assistants and alcohol/drug counselors—though these jobs may have industry certifications.
Higher educational and training requirements clearly affect the economic returns of available jobs. Figure 1 shows the ratio of median hourly wages for health occupations relative to the statewide median hourly wage for all jobs (about $27.30 in 2024). All the High category occupations garner median wages well above other jobs—with registered nursing and dental hygienist wages more than twice as high. Some occupations in the Medium category also provide higher wages than the typical job, in particular LVN and psychiatric techs. In the Low category—jobs that require the least amount of training—typical wage levels are below that of most other jobs in the state.



Those newly entering these professions may not initially earn median wage levels, given they have relatively less experience than others in the profession. Moreover, wages vary regionally to some extent and across employers. We explore these dimensions in the next section, including how completion of health credentials affects earning trajectories at the individual level.
Returns Vary Considerably across Different Programs
Health career training programs are by far the most remunerative at community colleges relative to other career education fields (e.g., business, information technology, child development). Associate degree programs in health can even translate into larger economic gains than bachelor’s degrees in many majors (Cuellar-Mejia et al. 2025). Figure 2 shows how these results are driven in large part by high returns from associate degrees in nursing and associate degrees in certain allied and dental fields, including radiologic technology and dental hygienists—all affording wage gains of 90 percent or more.



Other programs that typically result in long-term certificates also offer substantial gains—e.g., for students completing LVN (37%), paramedics (32%), and psychiatric technician credentials (43%), and to a lesser extent dental assistants (28%). By and large, short-term credentials result in much smaller wage gains, if any, relative to what individuals would have likely earned without completing the training program. Still, these credentials can increase the likelihood of employment and provide entry into jobs in the health care sector that could have longer-term career potential. Certain industries or employers within the health profession—hospitals, for example—have many different high-wage jobs and long-term training opportunities for advancement.
Present changes in the health care sector from federal policy along with state minimum wage law in California, which establishes a higher minimum wage for jobs in several health care settings, could affect earnings potential, job availability, or both. It will be important to track changes in earnings potential for these health care occupations since it matters crucially for the state’s ability to recruit a future workforce—and for present and future workers to meet their economic needs.
Earnings Gains Also Vary across Demographic Groups
Our research finds differences in earnings returns from health credentials across student groups (Figure 3). Men see smaller gains from completing health programs at the community colleges compared to women. Relative to their earning trajectories in the five years prior, men who complete a health credential increase their earnings by about 60 percent within six years compared to women, whose earnings increase about 71 percent on average. Across racial/ethnic groups, white students experience the largest returns—earning nearly 75 percent more than they would have been expected to if they had not completed the health credential. In comparison, Black and Asian students see smaller earnings gains—about 55 and 58 percent, respectively. Latino students earn about 63 percent more on average.

In part these earnings gaps reflect the types of programs different student groups pursue and complete, which we probe further in a later section. However, even when we narrow in on specific student groups who earn an associate degree in health (most are ADNs), we see similar gaps in wage returns across demographic groups (Bohn et al. 2019). Other factors like access to different health care jobs (and the wages or hours they offer) as well as personal preferences for work intensity may also play a role.
These gaps could also be driven by differences in the industry settings where people find work. Hospitals are the primary employer for several occupations—including registered nurses, respiratory therapists, radiologic techs, and psychiatric techs (Technical Appendix Figure A2). Long-term care facilities like skilled nursing and home health care are the primary industry for CNA and LVN jobs, though they have some opportunities in hospitals (about 30% and 15%, respectively). Most medical assistants and dental occupations—including dental hygienists and assistants—work in outpatient settings such as doctor and dentist offices or community clinics. Most EMTs are employed in the ambulatory care services industry, while pharmacy techs are most often employed in non-health industries, such as retail stores.
When we look at differences in wage levels across industry settings, we find three of the four occupations with the highest returns and median wages are primarily employed in hospital settings (Technical Appendix Table A3). Registered nurses and radiologic techs who work in hospitals have median hourly wages several dollars higher than for the occupation overall. There are not many notable differences among other occupations that require less training and command lower wages. Licensed vocational nurses and CNAs earn slightly less in long-term care settings than other industry settings. Interestingly, psychiatric techs earn less in hospital settings than other industry settings, which may be driven by financing constraints of publicly funded psychiatric hospitals or low reimbursement rates for mental health services more generally.
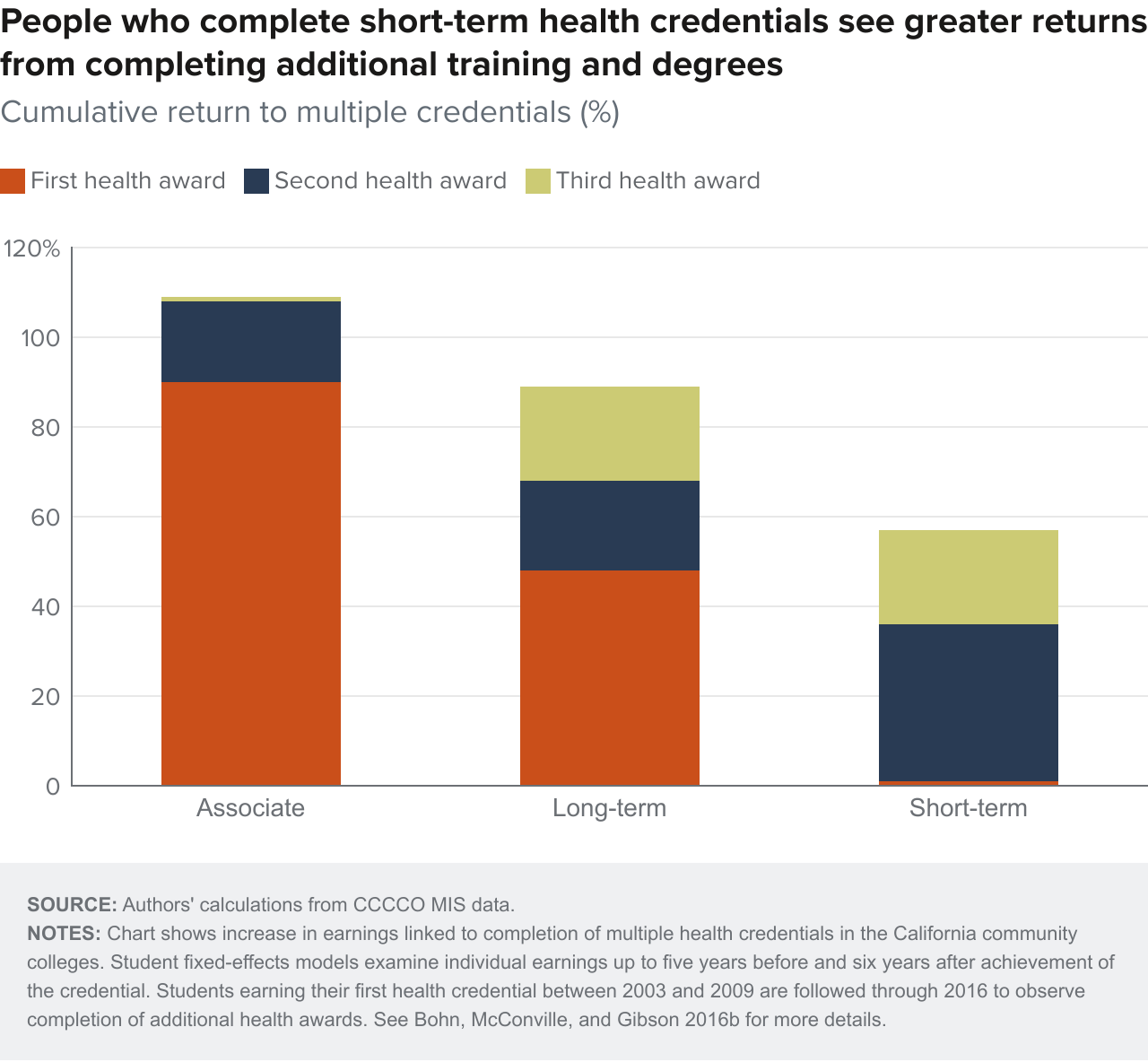
Additional Training Can Result in Longer-Term Gains
Some health fields offer the potential to stack credentials—that is, complete a short-term training program, gain work experience, and return later to build additional skills and complete higher-level degrees along a career pathway. For example, in nursing there are training pathways to move to increasing responsibilities that can dramatically increase earnings. Students can progress toward registered nursing jobs by first completing programs such as CNA and LVN.
As Figure 4 demonstrates, students who initially complete a certificate at the community colleges see higher earnings mobility by completing additional credentials (Bohn et al. 2016b). This is consistent with other recent studies that find higher economic returns from stacking community college credentials in health fields (Meyer et al. 2025; Daugherty et al. 2023). For those who complete a long-term certificate, obtaining a second and third credential increases wage returns by 20 percent for each additional award. This essentially allows them to catch up to the wage gains of those who initially complete an associate degree in health—though it takes longer to realize those returns. Stacking credentials is especially important for those who initially earn a short-term health certificate, which confers little in terms of wage gains. Earning a second health award increases earnings by 35 percent, and completing a third award adds another 20 percent to wage gains.
More than half of people who initially earn a short- or long-term certificate in a health program return to the community college system within three years to complete additional coursework. However, only about 20 percent complete a higher-level health award (e.g., “stack” credentials; Bohn et al. 2016b). It is possible that rates of successful stacking—in particular along a nursing pathway—are increasing, as community colleges have made significant investments in strengthening those. Since stacking credentials takes students much longer, research to quantify changes in stackable pathway completion lags. Moreover, it is possible that some people complete a pathway by moving to private-sector training providers, which is not incorporated in our findings above. More work in this area is warranted and eventually should be possible with the build-out of the state’s Cradle to Career data system.
In our focus groups, both community colleges and nonprofit workforce organizations shared important information about making these opportunities available:
Our college works closely with adult schools in our area. They provide a CNA program that lets people start there then transition into community college programs like psychiatric techs or registered nursing that can get them jobs at local hospitals. –Community college career counselor
Students start with our CNA program, which typically is a pretty short program. Then they may start looking into our RN program, which is lengthier. It’s critical for these students to know exactly what resources we offer so that they can be ready to go into the careers that they are seeking—and even so that they know what careers are available for them. –Community college career counselor
So while quick entry to health careers via short-term credentials may be attractive, economic mobility could be limited over the long haul for those who do not know about longer-term training and career options or have the support of career counselors. Making the link between short-term credentials and longer-term pathways to more remunerative careers could be of particular importance for younger people as they make key choices on educational paths after high school.
Next, we turn to an examination of where Californians receive postsecondary training for health programs, and their costs.
Health Training Providers and Costs
Californians who want to pursue health training have several options. The state’s community college system is the primary public provider of career education and job training. Across the 116 colleges, more than 25 different health programs are available to prepare people for a range of occupations in the health care sector. For the occupations we focus on in this report, about 40 percent of sub-baccalaureate credentials earned in the 2022–2023 school year (most recent year of data available) were through community colleges (Figure 5). The other 60 percent were from private for-profit institutions. Most for-profit health credentials were long-term certificates requiring between 30 and 60 units, which can be completed in one to two years in a few select health programs. These include medical assisting, dental assisting, and LVN.



As previously discussed, about half of registered nurses have at least a bachelor’s degree when they enter the workforce. Nonetheless, community college nursing programs provide a low-cost option across all regions of the state for completing an associate degree in nursing, which qualifies people to become licensed to work as a registered nurse. And there are efforts to expand applied bachelor’s degrees at community colleges to include BSN programs.
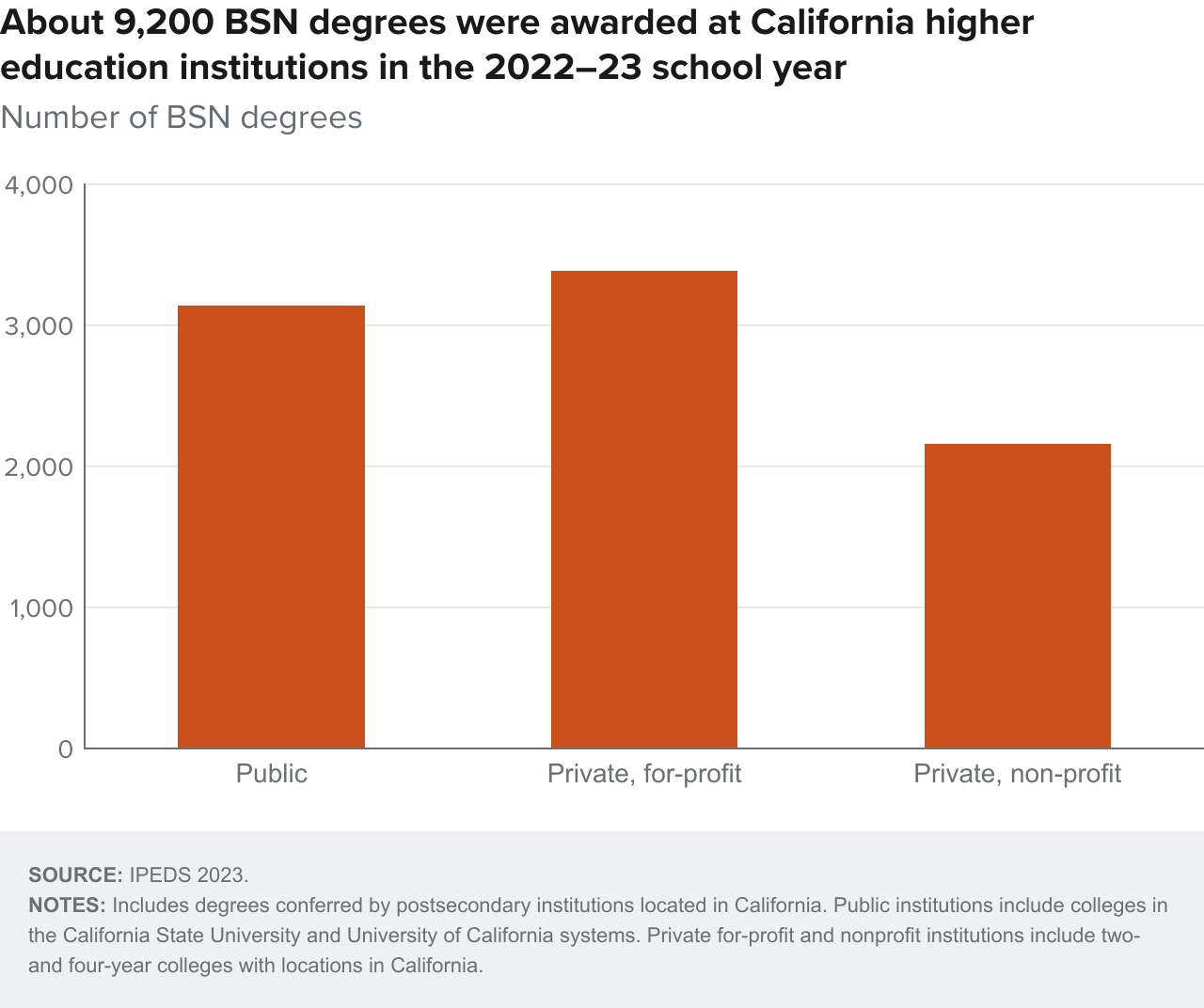
Across all California postsecondary institutions, more than 9,000 BSN degrees were conferred in 2022–23 (Figure 6). About 3,100 were completed at public universities, primarily the California State Universities and a few University of California campuses. Private for-profit colleges awarded about 3,400 BSN degrees and private nonprofit colleges about 2,200. We do not know how many of these degrees were completed by registered nurses who may have started with ADNs. Programs are available for registered nurses to complete a BSN in relatively short timeframes.
Despite for-profit institutions being a major health training provider, they are not the primary focus of this report in part because they are not funded by public investments (though federal financial aid is a key source of funding) and they do not offer as many different health programs relative to the community college system. In addition, information on enrollments and outcomes for students is much more limited. Still, they are a key player in the training ecosystem and affect the choices some health students have, especially for certain pathways—including medical and dental assisting, LVN, and registered nursing. Where data permits, we provide information on health training in for-profit colleges as important context.
Figure 7 shows the distribution of sub-baccalaureate health awards completed at California public institutions—almost all community colleges—and private for-profit colleges (private nonprofit colleges confer very few sub-baccalaureate health awards). Much higher shares (70%) of Black and to a lesser extent Latino (60%) students who earn awards in health fields do so at for-profit institutions. Most of these awards are long-term certificates and just over 10 percent are associate degrees. In comparison, about 60 percent of white students and over half of Asian students complete health credentials at the community colleges. Some of this may reflect differences in where students of different racial/ethnic groups live in relation to available training opportunities. Research evidence suggests higher concentrations of for-profit institutions impact students choosing those programs, and in particular, students from more disadvantaged backgrounds (Chung 2012).

Training for a few of the occupations we discuss here can be accessed through nonprofit workforce organizations. These organizations are often funded by public workforce development programs, like the federal Workforce Innovation and Opportunity Act (WIOA), that support training for people with barriers to employment. A comprehensive evaluation of California workforce training programs found that most boost employment prospects and several also increase earnings levels (Rothstein et al. 2022). Often, health training at nonprofit workforce agencies tends to be short-term programs that prepare people for roles such as nursing, medical, or dental assistants. Unlike most health programs at community college or for-profits, they also do not always confer college credits, though workforce agencies may partner with community colleges for some programs. Additionally, a few community college health offerings have non-credit options more comparable to training offered by workforce development nonprofit organizations. Community college initiatives to offer credit for prior learning could enable people who complete health programs at nonprofit agencies to receive college credits if they are interested in pursuing additional training.
Finally, it is important to note that we do not know how often individuals combine training across different types of providers. For example, people can complete training for a nursing or dental assistant at a nonprofit workforce agency and then move on to either for-profit or community college programs for LVN or dental specializations. Likewise, people may complete CNA programs at community colleges and then work toward an associate or bachelor’s degree in nursing at private nonprofit or for-profit institutions. More integrated workforce and education data systems are being developed to better understand how people navigate across the various higher education and workforce systems available in California.
Costs of Health Training Programs
Program costs obviously contribute to the potential economic returns of health training—especially in the near term as people must pay off any loans they receive to pursue training. California community colleges have low tuition and many students can attend for free due to fee waivers and grants—though total costs that account for things like housing and living expenses are much higher. Average annual costs of tuition and fees at California community colleges are less than $2,500 and are substantially lower than four-year colleges and for-profit institutions (Zhou 2024). Costs for health programs can be slightly higher. For example, according to the Bureau of Registered Nursing, registered nursing programs average about $4,000 per year and LVN costs about $3,000. Program costs for short-term training at the community colleges are even lower since many of these programs can be completed in less than a year.
For-profit institutions—which, as we see above, confer the majority of sub-baccalaureate health credentials in the state—are much more expensive and tend to serve higher shares of older students and those underrepresented in higher education (Cellini and Turner 2019). Costs of associate degree programs in nursing at California private, for-profit colleges are more than seven times the cost at the community colleges, and LVN programs are more than five times. Costs of medical and dental assisting programs—the other large health programs offered at for-profit colleges—are also high, averaging about $17,500 (see Technical Appendix Table A5). For some, the higher expense of for-profit institutions may pay off in convenience and efficiency, especially for students who have help paying for training through programs like union trust funds (McConville et al. 2021). But for others—and overall—the higher expense results in more student debt along with worse job outcomes (Cellini 2021).
California does offer financial assistance for many health training pathways. The California Department of Health Care Access and Information (HCAI) administers several scholarship programs that can defer education and training costs for people pursuing careers in many health care fields. In return, people who receive training grants commit to work in certain health care facilities and underserved communities for a certain period of time.
How and Why Do People Choose Certain Education and Training Programs?
Understanding how and why people select among available health training programs is paramount to improving potential for economic mobility. Much can be learned from one study of California community college students and a survey of students across a few colleges to assess how information about labor market outcomes impacts program choice (Baker et al. 2018). Combined, the findings indicate course enjoyment or interest is the most important predictor of major choice, followed by expected grades. Salary had a positive relationship with choice of major, especially once students were provided with accurate information about labor market returns.
These findings are consistent with what we heard from training providers when asked what they felt were the most important factors students considered when choosing a health training program:
What helps a student choose a program is knowing the certification meets industry standards so they can consider what kind of job are they going to get after they complete the program. – Community college career counselor
Probably the number one reason they say that they are choosing to get into health care is to help the community… Sometimes we have them take a career-focused assessment and part of their personality is the social, helpers personality. They’re helpful, collaborative, cooperative people—it’s part of their upbringing. – Community college career counselor
Moreover, a growing body of evidence focused on career education in high schools finds large differences in participation and outcomes by gender, race/ethnicity, and income (Ecton and Dougherty 2023; Bonilla 2020; Brunner et al 2021). These gaps could be driven by differences in student demand or interest in certain fields of study or by access to certain courses or programs—or both. One recent study of high school students in Michigan found participation gaps by gender were related to student interests—and were largely driven by more girls choosing health. Gaps by income levels, however, were influenced more by differences in access to programs, while gaps by race/ethnicity were impacted by a combination of both interest and access (Jacob and Ricks 2023).
The probability of choosing a for-profit college also seems to be influenced by socioeconomic factors—with students from low-income families more likely to choose for-profit institutions and those from middle-income families more likely to choose community colleges (Chung 2012). Furthermore, several rigorous studies have documented substantial substitution between community colleges and for-profit institutions for sub-baccalaureate education (Cellini et al. 2019). Research examines how changes in public investments for community colleges impact for-profit enrollments, applications, and closures. These studies find consistently that increased funding for community colleges reduces the likelihood of attending or applying to for-profit institutions, and conversely that declines in public investment in community colleges increase for-profit attendance (McGuinness 2024; Goodman and Volz 2021; Cellini, Darolia, and Turner 2020; Darolia 2013; Cellini 2009).
Along with the types of jobs students would be able to secure, the other main considerations training providers emphasized were the length of time the program took to complete and the costs:
I would say, for the participants that we’re serving, the attraction to our healthcare pathway program is that our programs are free and take about 12 weeks to complete. So people can start working towards getting skills quickly and connect to jobs that can hopefully lead to more financial security. – Nonprofit workforce provider
We start off with career and training exploration, which covers the length and difficulty of the training program. So the exploration really gives them the opportunity to understand what the commitment looks like. – Nonprofit workforce provider
Basically, our college is free for county residents. But I think one of the main factors students consider is whether they’re going to have access to any type of financial aid support. – Community college career counselor
Community colleges and nonprofit training providers alike devote resources to providing information on program expectations and requirements, as well as guidance on career pathways and connections to employment. All community colleges have resources devoted to career counseling services, many operating Career Centers with several counselors on staff to help guide students. In addition, the community college system invests in labor market research centers, which provide up-to-date labor market analysis and research to community colleges and regional collaboratives.
Who Pursues Different Health Programs at Community Colleges?
The evidence above demonstrates that the selection and completion of health training programs is critical to individual economic trajectories. Furthermore, some of the differences we observe in economic returns and types of training institutions may be related to the availability of programs at the community colleges (Cellini 2009; McGuiness 2024). As the main publicly funded provider of job training, California’s community college system plays a central role in health workforce pathways given their wide range of program options, low tuition costs, and locations throughout all regions of the state.
Enrollments in most community college health programs have recovered from drops during the pandemic, especially relative to overall community college enrollment—which is still down about 8 percent post-pandemic and projected to remain at lower levels over the next decade (Johnson et al. 2024). In the 2024–25 school year, there were more than 40,000 full-time equivalent (FTE) enrollments in these health programs (Figure 8). Because some students are enrolled part-time, this is likely an underestimate of individuals pursuing training.
Registered nursing dominates community college health programs, which have fully recovered from declines during the pandemic, with 2024–25 enrollments up 3 percent compared to the 2017–2018 school year. Enrollment levels in the three other high-return programs we study have also increased during this time period (14% for radiologic tech, 12% for respiratory care, and 8% for dental hygienists). Enrollment in shorter programs with low economic returns have also grown—and even more substantially—increasing about 30 percent for EMT and CNA programs and nearly 40 percent for medical assisting. In comparison, enrollments for LVN and psychiatric technician programs have declined during this time—down about 3 and 28 percent, respectively. Other medium-return programs like paramedics and dental assistants follow the overall trend of growing enrollment in recent years.



In general, community college program enrollments for these health occupations align with the distribution of statewide job opportunities (Technical Appendix Figure A2). For example, registered nursing comprises about 35 percent of total community college enrollments and credentials awarded in these health fields and a slightly higher share (38%) of jobs. For other occupations—including LVN, dental and nursing assistants, and pharmacy technicians—the share of jobs is also slightly higher than the shares of community college program enrollments and awards. EMT programs stand out as the second-largest community college health training after registered nursing. Program enrollments and credentials for EMT are much larger compared to the share of EMT jobs statewide, even if we include paramedic and firefighter jobs.
Next we examine demographic characteristics of students enrolled across different health programs at the community colleges.
More Women, Younger, and Latino Students Pursue Shorter, Low-Return Health Credentials
Younger students tend to do short-term training programs that lead to assistant-level, lower-return occupations (Figure 9). About 60 to 70 percent of enrollments in CNA, MA, pharm tech, and EMS programs are students age 24 or younger, similar to the age profiles of all community college students. These can allow students to start jobs and gain work experience more quickly than other, longer-term programs. The trend may reflect opportunities for stacking credentials, where younger students first engage with shorter-term assistant programs, work a few years, and then return to complete more training to advance. It also likely reflects recent investments and increasing career pathways from high schools to community colleges through programs like CTE Pathway Development Grants and Golden State Pathways (Bonilla & Thim 2025).



Considerably lower shares of younger students (25–30%) are enrolled in associate degree programs such as registered nursing, dental hygienist, radiological tech, and respiratory therapy. These programs have several prerequisites and are more selective in the sense that people must meet specific qualifications and be accepted into them. The years it takes to meet the requirements and secure an available program slot may contribute to the older age profiles of students.
Prerequisite courses can be a huge barrier because they have to get A’s and B’s. So I do get students who come to me because they got a C and they can’t move further. And then I suggest maybe you want to start off with the CNA program. And then try to retake that class while you’re waiting, because sometimes it takes 5 to 6 semesters for them to get into those programs they’re applying for. And having a CNA or LVN can increase their chances of getting into our registered nursing program. – Community college career counselor
These higher-return programs also often have waiting lists due to limited program capacity relative to the number of qualified students who wish to pursue training—for example, registered nursing has seen increasing numbers of qualified applicants in recent years. This has led to calls for increased training capacity at community colleges—and potentially adding applied bachelor’s degrees in nursing. Community colleges already confer bachelor’s degrees for dental hygienist programs—in the 2023–24 school year about 300 were conferred. There are also continuing efforts to expand BSN programs into the community colleges.
Older students may have additional responsibilities, whether family and child care and/or contributing to household earnings. Both can make it challenging to persevere through training programs. Our focus groups shared that child care needs were one of the most common reasons people were not able to start or complete programs:
The main problem we see is participants’ child care falling through. So when we do our interview process, we talk to them about having reliable child care and a couple of backup plans. Because with our programs being so short, there’s not a lot of makeup time. – Nonprofit workforce provider
I think the first year is the toughest, some of them are parents, they’re trying to juggle child care …they have a million things on their plate. – Community college career counselor
One program aimed at providing more intensive financial supports in the Los Angeles Community College district is providing universal basic income grants of $1000/month to students pursuing health programs.
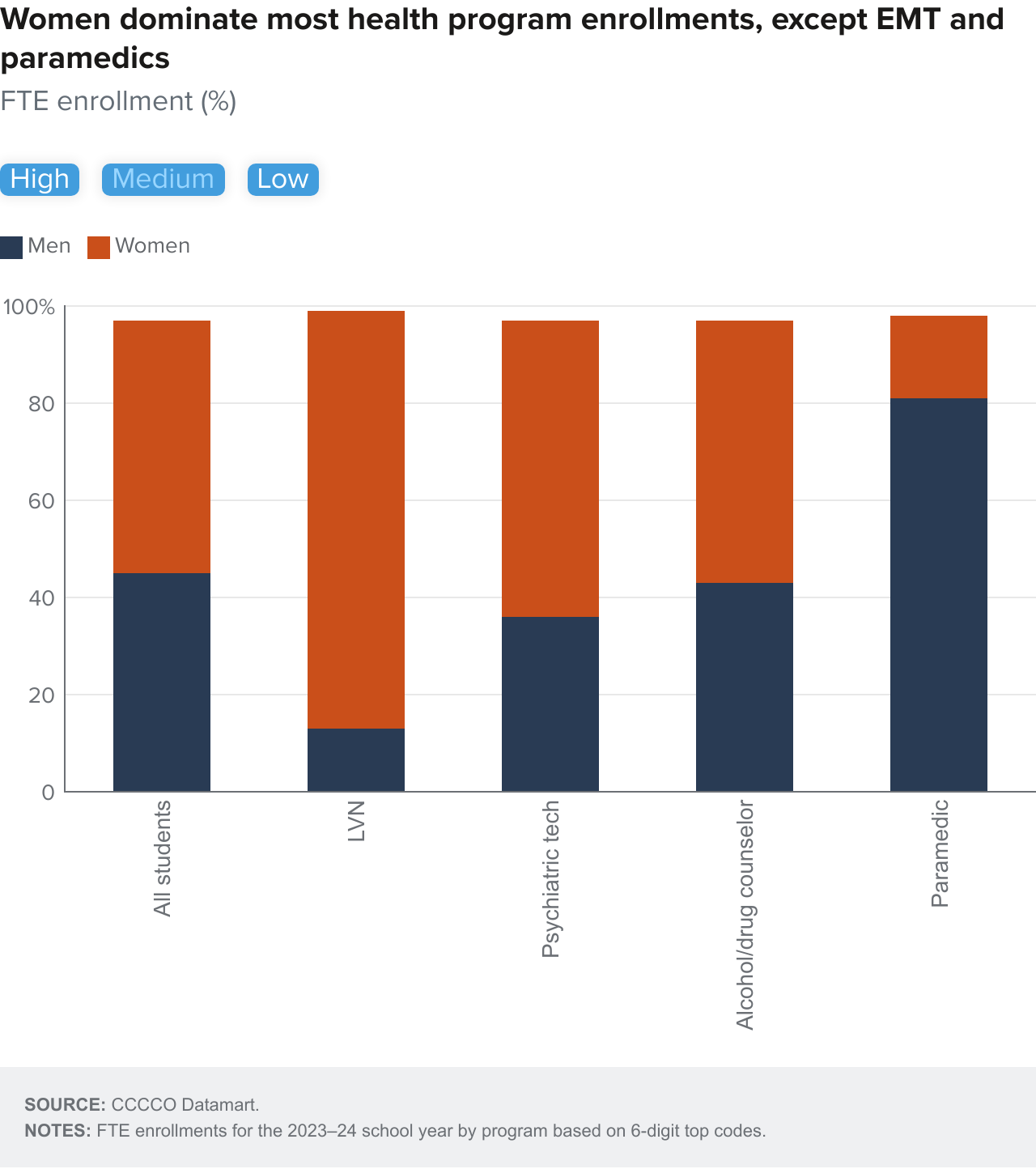
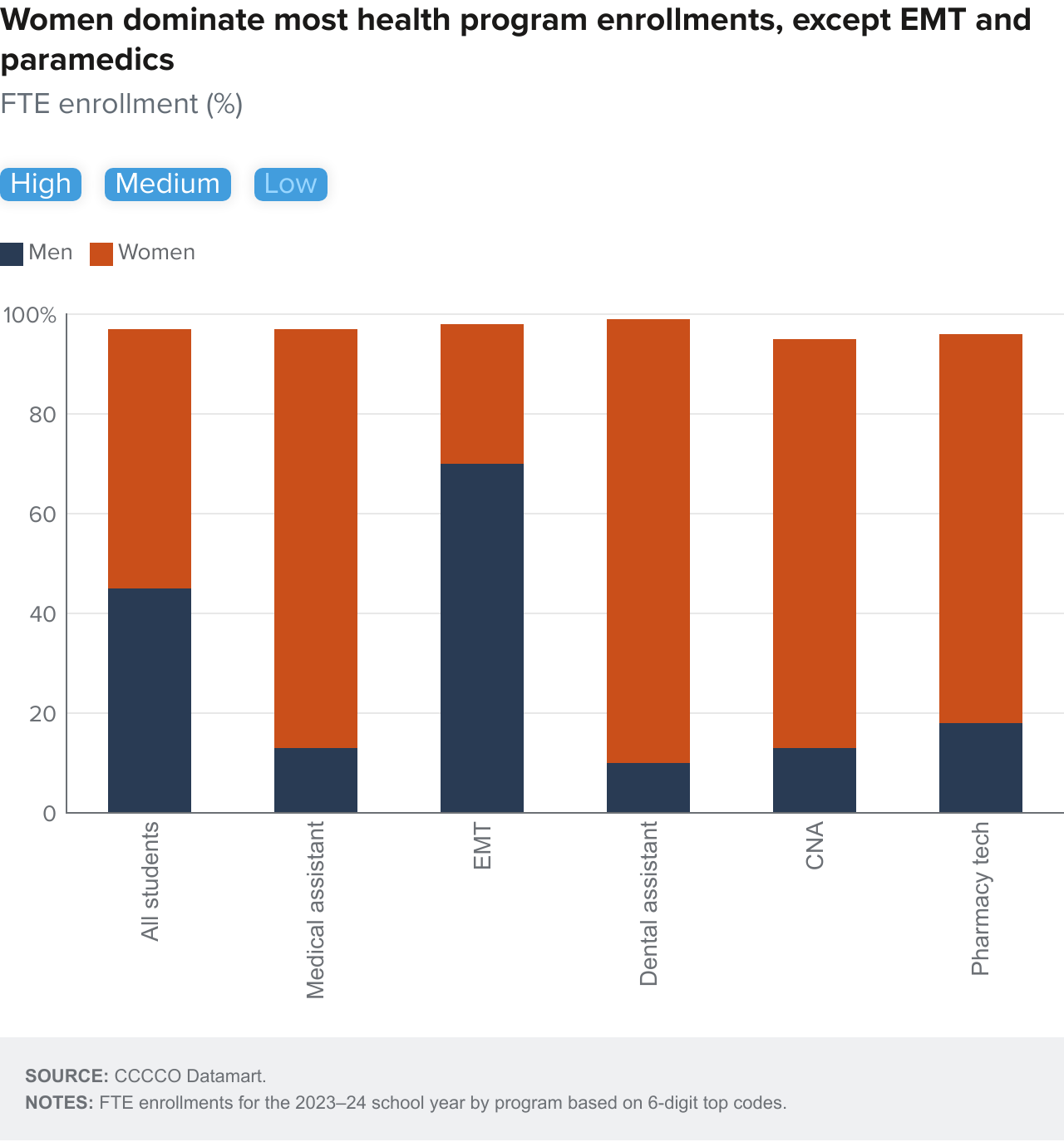
Women dominate most nursing and other health occupations we study and make up about 70 percent of total enrollments in community college health programs we study. Figure 10 shows the breakdown for the 2023–24 school year. In nursing, medical assisting, and dental programs, the share is even larger—nearly nine in ten students. Men comprise slightly higher shares of enrollments in registered nursing than other occupations—about 20 percent—but women still dominate overall. There are a few exceptions, most notably EMTs and paramedics, where more than 70 percent of enrollments are men. Certain tech and allied programs also have higher shares of men—about 35 percent of enrollments in radiologic tech and respiratory therapy programs. Behavioral health program enrollments, including psychiatric technicians and alcohol and drug counseling, also show higher shares of men relative to other health programs.
With the increasing economic returns on training for registered nursing and other allied health positions, there have been broad efforts to bring more men into the field. Still, longstanding patterns of occupational segregation remain in many health sectors, with women continuing to comprise the vast majority of workers in nursing and health care support roles.

As Figure 11 shows, relative to their share of all community college enrollments (62% vs. 50%), Latino students seem to be overrepresented in shorter-term training programs such as medical, nursing, and dental assisting and pharmacy techs. In comparison, about half of student enrollments in high-value associate programs including registered nursing, dental hygienist, radiologic tech, and respiratory therapy are Latino—about the same as total enrollments. Black students have considerably higher shares enrolled in behavioral health programs, while Asian students have higher shares in registered nursing and allied technical programs.
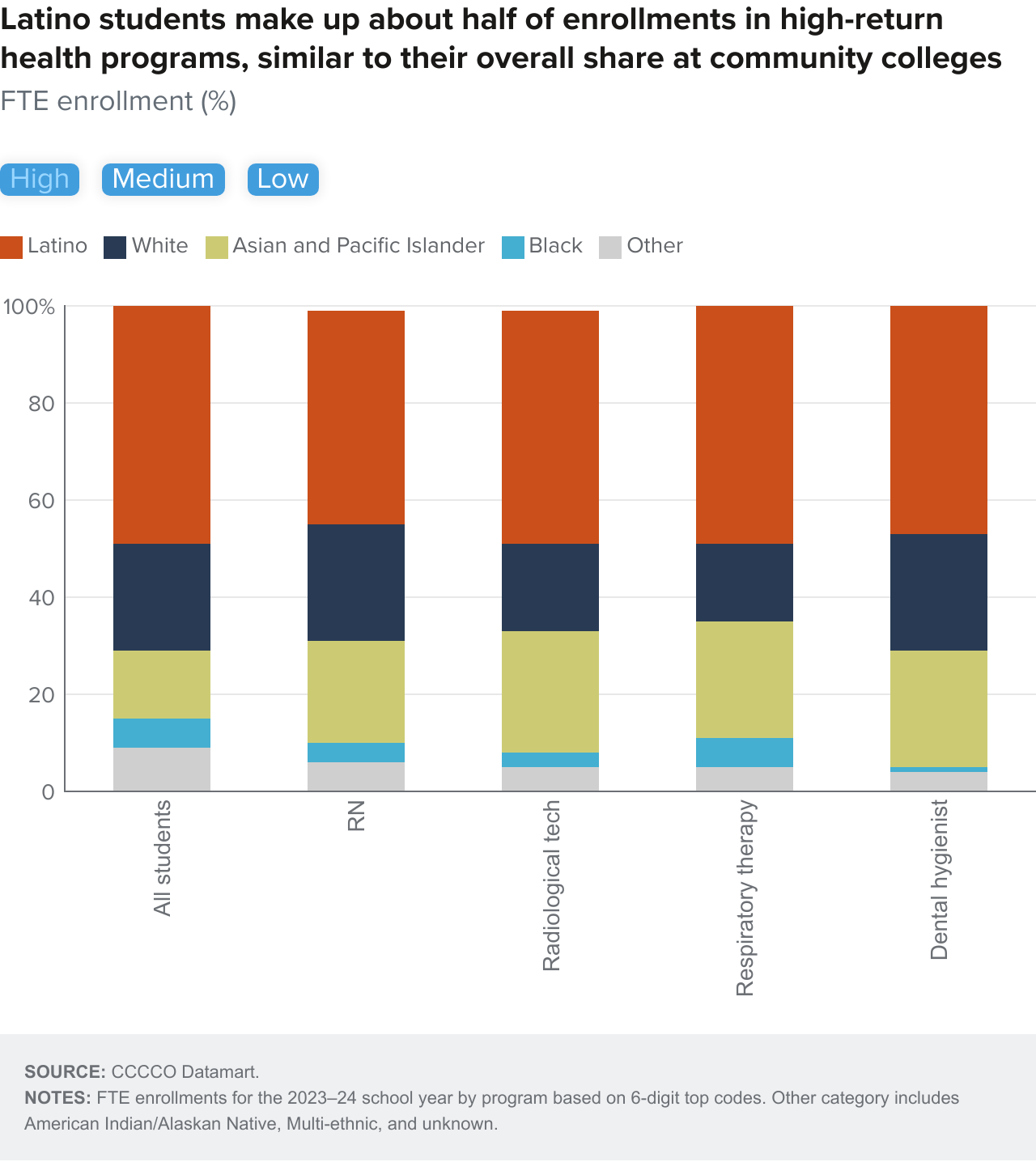


Expanding the diversity of the health care workforce to better align with the state’s population is a longstanding policy goal. The large growth in racial/ethnic diversity among California’s growing older adult population, who consume more health services, underscores this focus. Increasingly, older adults will be foreign-born and speak languages other than English (Johnson et al. 2025). Studies have documented that racial/ethnic and language concordance between providers (most often physicians) and patients can lead to increased trust and satisfaction and help bridge cultural gaps. In particular, providers that speak the same language can be key to reducing miscommunication and improving outcomes (Rittenhouse et al. 2021; Diamond et al. 2019).
Barriers to Improving Economic Opportunity via Health Training Pathways
The health training programs people choose have major implications for future job prospects. The regional distribution of available training programs may impact those choices along with student interest and local labor markets. In addition, many health occupations require people to complete an approved training program and obtain a state license to be qualified to work in the job.
Community College Health Program Offerings Differ across Regions
Some of the differences we observe in who pursues different types of health training could be related to the availability of programs across regions. Like K–12 public schools, community colleges are run by local districts that have latitude in making decisions about what programs to offer. This means that access in terms of geographic proximity varies across California communities. While relocating to take advantage of college or career training opportunities is possible, most community college students attend schools close to home.
Figure 12 shows how program enrollments vary dramatically across regions and across programs. Several regions, including the Central Coast, Kern County, the San Joaquin Valley, and the Far North, have considerably higher per capita enrollments in high-return programs than other regions. Registered nursing drives enrollment levels in high-return programs as the largest and most widely available throughout California community colleges. Several of these regions also have high enrollments in medium- and low-return health programs. Regions including the Inland Empire, Los Angeles County, and the Southern Border have fewer program enrollments per capita (which could be driven by their much larger population size). There seems to be less variation across regions in short-term health program enrollments that confer lower economic returns.



To be clear, just because there are programs available does not mean everyone can access them. In the case of selective programs like registered nursing or dental hygienist, prerequisite requirements may be a deterrent or obstacle.
Moreover, in the last several years, waiting lists at many community colleges also curtailed access. Our interviewees shed light on this issue:
They’ll apply to the nursing program here after finishing their two years of prereqs. They don’t get into the program. So they’ll just take a year off, and then that turns into two years, three years… then they have kids, and all these other responsibilities come up where they can’t get into the program. I can’t tell you how many people I have come in to reapply with the same story. Oh, yeah, I finished all my prerequisites for the program; I didn’t get admitted. And then life happened. It’s super hard for a student to come back full time to school once you take that gap. – Community college career counselor
A student tells me, I want to be a nurse, but I’m place bound. It has to be this college. I want to do my ADN program here. And it’s a lottery-based system, you know, and that’s just so tough for students, because they can’t even plan knowing which semester they’re going to be admitted into the nursing program. – Community college career counselor
The impaction of our nursing programs really limits student access and what happens is they turn to private institutions that have much higher costs and create more financial burden to get that nursing degree. – Community college career counselor
Lack of faculty and securing clinical placements for students are key challenges to expanding available training slots in nursing programs. A recent survey of registered nursing programs in California found that among those enrolling fewer students, about a quarter reported a lack of faculty as the most important reason and about 15 percent difficulties securing clinical placements (California Bureau of Registered Nursing 2024).
Challenges to Completing Community College Programs
Although completion rates in community college health programs are higher compared to other career education fields, many students still do not finish programs they start by earning a credential or degree (Bohn et al. 2016a; McConville et al. 2021). Completion varies considerably across health programs. Associate degree health programs included in this report boast very high completion rates, between 80 and 95 percent. On the other extreme, emergency medicine technicians have the lowest completion rates (around 40%) and only about half of students in other short-term programs like nursing assisting and pharmacy tech complete a credential (Bohn et al. 2016a).
We found that full-time enrollment is the strongest contributing factor to completing programs even after controlling for differences across gender, age, race/ethnicity, socioeconomic status, financial aid, and other factors (McConville et al. 2021). Still, some student groups fall off completion trajectories within the first few semesters of starting a program of study. This is especially true for Black students, suggesting that targeting intensive supports when people enter programs could be necessary to improve overall completion. In comparison, Latino students pursuing health pathways tend to have completion rates of their white counterparts, but it takes them much longer. In comparison, Asian students have the highest completion rates for community college career education programs though this may mask differences across Asian subgroups (McConville et al. 2021).
The length of time it takes to finish health awards at community colleges could be a factor in low completion rates. On average, it takes health students about two to three years to complete short- or long-term certificates. Additionally, community college health students often complete a significant number of units not necessarily related to their field of study, including in health training programs (McConville et al. 2021). This could reflect students’ need to maintain eligibility for financial aid by enrolling in general courses even if health courses are not available, their desire to work towards transfer, or being undecided about their specific pathway.
Our past work has shown students who receive financial aid—including Pell Grants, an indicator of students from lower-income families—are more likely to complete community college health programs and stackable credentials compared to those who do not. We also found that targeted support programs for student parents who received CalWORKs cash assistance increased the likelihood that students enrolled full time, successfully completed courses, and persisted to the next term (McConville et al. 2020).
Future Job Opportunities and Local Labor Markets
The regional distribution of health training programs is driven, at least in part, by local labor market demand. Even though they may also recruit from outside the local area, the presence of large employers like hospitals can create job opportunities—and training needs—for individuals in the region. Additionally, regional needs for health services driven by population growth and composition (e.g., aging) or policy (e.g., insurance expansion or contraction) also factor into job opportunities for prospective health workers.
The most recent state-level job projections suggest several of the health occupations we study here are projected to grow at rates above the state average (8.8%) by 2033, though there are some exceptions. Projected growth for LVN and CNA jobs is slightly lower than the state overall (8.3% and 8.4%, respectively) as are growth rates for dental assistants and dental hygienists (7.7% and 8.3%, respectively). Growth rates range from 10–20 percent across the other health occupations considered in this study. In addition to growing as a share of the workforce, job openings will also become available because of retiring workers or due to the turnover of workers in some occupations. Job openings are projected to be greatest for registered nurses (20,800 per year through 2033), but after that are expected to be more numerous in lower-wage occupations like nursing and medical assistants (between 15,600 and 17,000 per year) (Technical Appendix Table A6).
To assess how projected workforce needs match up with available and newly trained workers, we draw on a variety of sources. According to the Health Care Resources and Services Administration (HRSA)—a federal agency within the US Department of Health and Human Services—EMTs and respiratory therapists already have more workers relative to available jobs in California and that mismatch is expected to continue over the next decade (Technical Appendix Table A6). Similarly, supply-demand projection models from the California Department of Health Care Access and Information (HCAI) indicate the state has an oversupply of LVNs now and in the near future.
Nursing occupations—especially registered nurses—are the most widely studied and available. In collaboration with UCSF researchers, California’s Board of Registered Nursing (BRN) provides detailed estimates of the supply and demand for nursing professions. Their most recent statewide forecasts suggest a small, current shortage of RNs that will likely abate over the next few years (Spetz 2024). This implies a more balanced supply and demand for registered nurses statewide than the HCAI estimates for RNs, which forecast a shortage over the next decade.
While state-level assessments of workforce needs are useful for high-level planning decisions, labor markets operate at a local level, so regional projections are more informative for training providers and students alike. Depending on the source, forecasts for registered nurses are either relatively balanced through 2035 or face some shortages, which are more acute in certain regions. In particular, the Bay Area, Central Valley, and Central Coast regions are expected to have lower ratios of registered nurses than other regions, and less than national benchmarks suggest (Spetz 2024).
In response to the over- or under-supply of workers in any given occupation, employers adjust wages. Prospects of job openings as well as higher wages for an occupation may incentivize residents to pursue that career. However, in the health sector wages may not be as flexible as in other industry sectors because of financing through government programs and minimum wage policy in some fields (such as medical assistants and CNAs in some health care settings). Nonetheless, there is variation in wage rates for health occupations across regions in California, which to some extent reflects the supply and demand of workers.
We find that there is some variation in earnings potential across regions, but the larger variation is across occupations—consistent with what we presented earlier in this report. For instance, the highest-return occupations like RNs and dental hygienists earn between 1.9 and 3 times the median hourly wage across all regions of the state (lowest in LA and Kern and highest in the North San Joaquin regions—see Technical Appendix Figure A4). Medium-return health occupations earn between 0.9 and 1.7 times the regional median hourly wage, with LVNs being at the top of that range across all regions, and the biggest advantage to psych techs in the San Joaquin regions. Most other occupations earn roughly on par with median workers in their regions, or some slightly behind par, like EMTs and nursing assistants who earn 80–90 percent of median wages in some regions.
Licensing Requirements
As previously mentioned, most of these health occupations require workers to have a state license; medical assistants and alcohol/drug counselors are exceptions. While licensing requirements ensure that workers in jobs have adequate training and skills, they can limit access to many occupations and impose costs (Nunn 2018). In order to get a license to work in these health care jobs in California, one must typically pass a licensing exam, pay a fee, and meet other requirements like criminal background checks.
Passage rates for the national registered nursing exam (NCLEX-RN) are generally high, averaging above 90 percent for many available RN programs. Still, for those students who complete a registered nursing program and are not able to pass the licensing exam, the time and costs of training will not translate into the expected economic gains. Rates of passage for other health occupations are also relatively high but vary across different programs and institutions. Some training providers offer innovative ways to support their students who need to take licensing exams:
We coordinate to get private testing dates for the CNA licensing exam. So they can go as a class if they want and most of them do. And if you want the support of your professional development instructor being there, we have set that up too. We’ve paid for it, and we’ll get you through it. – Nonprofit workforce provider
Though licensing for health occupations is billed as important to protect public health and safety, there have been calls to reexamine California licensing requirements to help improve access to jobs and economic mobility (Little Hoover Commission 2016). In addition, most licensing exams are only offered in English, which could also create barriers for some people. Industry organizations representing skilled nursing facilities have lobbied for changes and introduced legislation to offer exams in Spanish or provide other accommodations for students whose native language is not English.
Conclusion
Health careers can provide economic gains and security for workers even if they do not have a four-year college degree—and at the same time provide essential needs for state residents. For both reasons, developing training pathways for and broadening access to sub-baccalaureate health careers are goals state leaders have articulated, from community colleges to the state legislature and governor’s office. In every region of the state, community colleges offer training to people that can prepare them for health care professions.
While there is no question that high-quality, accessible health care is essential for the population, the trained workers who provide care vary dramatically in their earnings potential and job prospects. Earnings are highest for registered nurses, dental hygienists, and radiologic techs. Among these, radiologic techs are projected to have the highest growth rate over the next decade, but registered nursing will have the most job openings. At the middle range of earnings are LVN, paramedics, and psychiatric tech occupations, for which Californians can complete training more quickly. Demand for these occupations is expected to grow, though some occupations—for example LVNs—are already training a sufficiently large number of workers. Shorter-term training in health for positions like nursing and medical assistants confers much smaller returns, though as an entry point to the profession, these opportunities may make sense as stepping stones to longer career pathways.
In light of these realities and given what we observe about the Californians who pursue sub-baccalaureate health training, a few key considerations for policymakers and practitioners are evident:
- People pursuing health career pathways need accurate, actionable information about training requirements and job opportunities early on in their educational trajectory. Choosing to pursue postsecondary training in health programs can be good for long-term career outcomes, and early exposure to career training supports that. But the choice of which credential to pursue can have long-term consequences. Some offer high earnings returns earlier but extend the time it takes to complete the training. Others offer lower returns early, with the opportunity to accrue additional credentials needed for advancement later.
- Supports for completing career pathways, especially if they involve multiple credentials, could help more individuals in health careers advance. Many people stop their educational journey in health at the community colleges with short-term credentials that offer only small advancement economically. In our interviews, financial support and capacity constraints were the most frequently mentioned barriers for connecting people to high-return programs in health. With these in mind, increasing flexibility in how, when, where, and how much such training is delivered in community colleges could help interested students advance—and could help some students access training through community colleges versus private, for-profit colleges.
- Reliable information about future hiring is essential for educational institutions and individuals alike. In a period of substantial demographic, economic, and health policy change, it is difficult to project exactly how many future workers will be needed. But broad trends can nonetheless foretell some dimensions of what future job opportunities will look like for Californians in sub-baccalaureate health occupations. Statewide coordination—for example through California Jobs First and the Master Plan for Career Education—could support alignment between industry and educational institutions. The regional aspects of those plans, and collaboration between local employers, educational institutions, and workforce stakeholders are also essential to ensure that opportunities for students come to fruition. Health-specific collaboration that includes licensing boards and supports workforce projection models can help plan for state training needs and investments.
There is great promise in bridging health workforce needs for California’s population and workforce opportunities for individuals in search of economic security and mobility. The state’s health workforce is substantial and growing, with higher growth expected in many occupations that do not require a bachelor’s degree or more. Health workers are essential in all parts of the state, even those where high-paying jobs for workers without a bachelor’s degree are sparse. However, as we have shown, there are notable distinctions in the earnings potential within that set of sub-baccalaureate health occupations. Those workers require a clear sense of their health career potential so they can match that with their expectations and investments in training. Providing it is key to meeting current and future workforce needs while improving economic security.
Topics
Economic Mobility Economy Higher Education Jobs and Employment Workforce and Training Workforce Needs